
Impact of Environmental Sanitation and Hygienic Practices on Nutritional Status of Lodha Women and Children of West Bengal, India
Abstract
Aim
To assess the sanitation and hygienic practices of women and its effects on the nutritional status of the mother and preschool children of the Lodha tribal community in two districts of West Bengal.
Methods
A cross-sectional study was conducted during November, 2014 - December, 2018 of 941 Lodha mothers and 1043 of their preschool children in Paschim Medinipur and Jhargram districts. All information was collected by using KAP questionnaire following interview and group discussion. Mother nutritional status was assessed based on body mass index (BMI) and mid upper arm circumference (MUAC). A child was classified as underweight, stunting and wasting as weight-for-age, height-for-age and weight-of -height Z-score below -2 standard deviation of WHO standard.
Results
This study found 35% of the households used safe drinking water. Almost 97.2% of the mother had the low hand wash score and about 67.1% of them had an average WaSH score. Overall, 41.6% and 1.6% mothers were suffered from undernutrition (BMI <18.5 kg/m2) and overweight/obesity (BMI≥25kg/m2). Whereas, 48.9% women were undernourished based on MUAC<22.0cm. Moreover, the overall prevalence of wasting, stunting and underweight of preschool children was 31.9%, 62.1% and 61.3%, respectively. The WaSH score of family was significantly associated with child stunted and underweight.
Conclusion
There is a good association between poor household WaSH practices with child undernutrition and morbidity. Hence, there is an urgent need to develop the comprehensive knowledge, attitude and practice (KAP) guidelines in their language to educate them about appropriate water storage, retrieval methods, sanitation and hand washing practices.
Author Contributions
Academic Editor: Sasho Stoleski, Institute of Occupational Health of R. Macedonia, WHO CC and Ga2len CC, Macedonia.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Prasanta Sabud, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have no conflicts of interest to declare.
Citation:
Introduction
Clean and safe water for drinking and hygienic sanitation remain two of the simplest and most significant needs of the individuals for their wellbeing. Billions of people around the world, mostly in underdeveloped and developing countries, are deprived of safe drinking water, improved sanitation, and used to much un-hygienic behaviour. A report estimated about 2.3 billion and 2.5 billion individuals’ globally secured access to drinking water and better sanitation, respectively. Still, one billion people are accustomed to open defecation, and 748 million people have no access to safe drinking water, and a lot of millions of people have no access to soap and water to wash their hands 1.
Admittance to safe water, sanitation and hygiene (WaSH) has momentous functions in poverty alleviation and financial advancement of a nation 2. As indicated by WHO, each and every dollar paid on WaSH brings a return of $5.50, in the way of lowering health costs and prevalent profitability 3. Moreover, individuals living without admittance to a latrine additionally face outrage in pooping the open spot, with the dangers of various constant illnesses and even maltreatments, generally for women and girls 4.
In India, practices of improved WaSH are not satisfactory, and when it comes to rural areas, particularly among the tribes the overall situation is far more critical. They became more vulnerable from both health and economic aspect when they have poor hygienic practices, wash hands improperly 5. These vulnerable populations would be at risk of suffering from waterborne diseases like diarrhea, cholera, typhoid, especially among children and elders, which are preventable 6. Globally, diarrhoea was the eighth leading cause of death among all ages in 2016, 7 and presently, COVID-19 is going to place in the top rankings.
In India, still have some tribal communities trying to be integrated and adopted a mainstream culture for their existence. But this process of integration has presented another set of challenges to underprivileged communities. Lodha tribe, a Particularly Vulnerable Tribal Groups of West Bengal is one of them. They are among the indigenous tribes who are mostly living in isolation in the forest fringe areas of Jhargram and Paschim Midnapore districts of West Bengal. They are mostly landless, marginal laborer otherwise dependent on forest produce, has no adequate income and food security. The latest census signified that, they have many health issues than the rest of the Indian population and thus they are vulnerable 8. The underlying causes of ill health of any population may be due to their poverty, malnutrition, lack of education and poor environmental hygiene 9. WaSH practices of non-tribal people in India has been documented by some of the study 10, 11, 12; but still there remained a paucity of information from the India's tribal population about this relevant issue. The objective of the current study was to study the water, sanitation, and hygiene practices of the Lodha Tribe in Paschim Medinipur and Jhargram districts of West Bengal, India.
Materials and Methods
Study Design & Selection of Subjects
The cross-sectional study applied quantitative and qualitative methods. In the quantitative method, one to one interviews and observation checklists were conducted in a sample of 941 households selected by random sampling method. In the qualitative component, focus group discussion and key informant interviews with the local authorities and village elders were conducted.The study was conducted in the 49 villages of Paschim Medinipur and Jhargram districts of West Bengal, India. In each sample village, at least 10 household and one key informant were interviewed following questionnaire method.
Sample Size

Ethical Considerations
The objectives of the study were informed to the local community leaders and the relevant authorities. A consent letter (the contents of the consent letter was read and explained to the woman) was collected from each woman for her interview and measurement prior to this field work. Ethical approval (vide letter no. IEC/10/2/C-2/18, dated 20-04-2018) was obtained from the human ethical committee of Vidyasagar University, Midnapore, West Bengal, India.
Assessment of Socioeconomic Status (SES)
Socioeconomic status of household was assessed by Kuppuswamy Socioeconomic status scale 13.
Measurements of Anthropometric Parameters
Height, weight, mid upper arm circumference of mothers (MUAC) and childrenheight and weightwas made and recorded following standard procedure 14. Mother nutritional status was assessed based on BMI international classification as undernutrition (BMI<18.5 kg/m2), normal (BMI: 18.5-24.9 kg/m2) and overweight including obesity (BMI: ≥25 kg/m2) and Mother MUAC value of <22 cm and ≥22 cm is considered as undernutrition and normal, respectively 15, 16. Anthropometric indices of the children were wasting, stunting and underweight calculated by WHO anthro software according to the WHO Growth Child standards 2006 17. A child was classified as underweight, stunting and wasting as weight-for-age, height-for-age and weight-of -height Z-score below -2 standard deviation.
Measurements of WaSH Parameters
The researcher has developed this method to assess women's knowledge on nutrition. The method consisted of 15 multi-choice questions. Every right option was scored one, and every wrong option was scored zero. Knowledge score was arbitrarily graded as good knowledge: 11-15, average knowledge: 06-10 and poor knowledge: 0-5. WaSH score was calculated from the total of the four specific indicators; drinking water score (0-6 points), sanitation score (0-3 points), hygiene score (0-5 points), and hand washing score (0-12 points) and had a total of 26 points possible as recommended by Reddy et al 18.
Data Analysis
Chi square test was performed to assess group differences in knowledge score and WaSH score with the socioeconomic status variables (education, income, number of family members, type of house, number of children, latrine facility, availability of safe drinking water etc.) and nutritional status of mother (BMI and MUAC) and children (underweight, stunting, wasting). Logistic regression analysis was conducted to determine the variables associated with diarrhea form of morbidity (within 15 days of the survey), WaSH score and a Knowledge score of respondent mothers. All statistical analyses were performed using the SPSS Package 21. Statistical significance was set at p less than 0.05.
Results
General Information
This study engaged both respondent mother (n=941) and their preschool children (n=1043; 533 boys and 510 girls) of the Lodha community in Paschim Medinipur and Jhargram districts of West Bengal. The majority (63.2%) of the mother was the resident of Paschim Medinipur district. Almost two third (66.7%) of the respondent families were nuclear comprising single parent. The average family size was 4.5± 1.42. The majority (92.8%) of the mothers were aged less than 30 years. Only 23.2% mother was literate and most of them were primary dropped out. Literacy and income of the husband were also dismally low. The respondent mother contributes to family income also look after the children and family chore. They are mainly engaged as agricultural laborers. According to Kuppuswami Socioeconomic status (SES) scale, 98% respondents belongs to a lower SES class (Grade-IV of the SES scale). Most of the houses of Lodha families were ‘Kutcha’, made of mud and straw-thatched. Only, 6% families had ‘Pucca’ house made of brick wall and asbestos in the roof.
Drinking Water Sources in the Village
About 35% of the respondent families get their drinking water from clean and safe water sources (hand pumps or protected wells or piped water supply) throughout all season. Only 2% of the family had drinking water at their premises. Safe water sources (public or private) have been available usually within 5 minute walking distance from the house. Predominantly women (84%) collected water for everyday use in the household from outside (Figure 1).
Figure 1.Water collector of Lodha family
Water Storage
About 37% of the respondent families use metal pot, 30% clay pot and 2% of the families use jerry-cans, 31% use plastic buckets and pots for storage of drinking water (Figure 2). It was observed during the survey that these water reservoirs were often without lids. Almost all respondent mothers (90 percent) habituated to take water by dipping glass in water pots.
Figure 2.Material of water container for Lodha family
In general they used to wash the drinking water containers by using water only. Almost, 14% of the respondent mothers used detergent and otherwise use ash or clay for this purpose. The respondent mothers wash their drinking water containers during fetching every time (77%), every day (14%) and whenever it stayed dirty (5%). (Figure 3) No households of the respondent mothers had ground and rooftop water tanks and don't have any home filters. Running water tap has been installed in some village pockets, but there were issues of safety and quantity.
Figure 3.Frequency of cleaning water container by Lodha family
Domestic Water
Generally households uses bore-hole water, shallow well, pond or river water as domestic water like cleaning, cooking, and personal hygiene etc. But these sources are scarce during the summer season.
Wastewater
The respondent households were not connected to a waste water network. Sewage accumulation is worsened during rainfall.
Defecation Practices
Open defecation was the predominant practice among these families (96%) and the rest (4%) use traditional latrine (pit latrine with slab) for defecation (Figure 4). They have no place for such building and they did not have money for the constructing a standard latrine. The majority (89%) of Lodha mothers thrown children stool at nearby bush (Figure 5).
Figure 4.Defecation Practices of Lodha family
Figure 5.Handling of children stool by Lodha family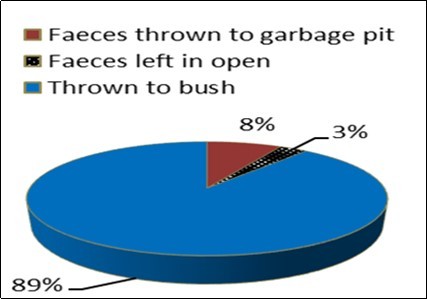
Solid Wastes Management
Community-generated solid wastes gathered nearby areas as household waste is thrown into the bush/garden (Figure 6). Open burning was ensured by young children and elders occasionally.
Figure 6.Solid Waste Management of Lodha family
Hygiene
The respondent mothers did not wash their hands before eating and cooking every time (Figure 7). Hand washing after defecation is performed predominantly by water only (56%). About 24% of study participants reported utilizing soap and water after defecation (Figure 8). The study participants' household members reported washing their hands with water only pre and post meals. Soap was used when it was felt the hands were being dirty. Only, 3.5% of study participants, the hand wash score was higher than five.
Figure 7.Material used for hand washing after defecation by Lodha family.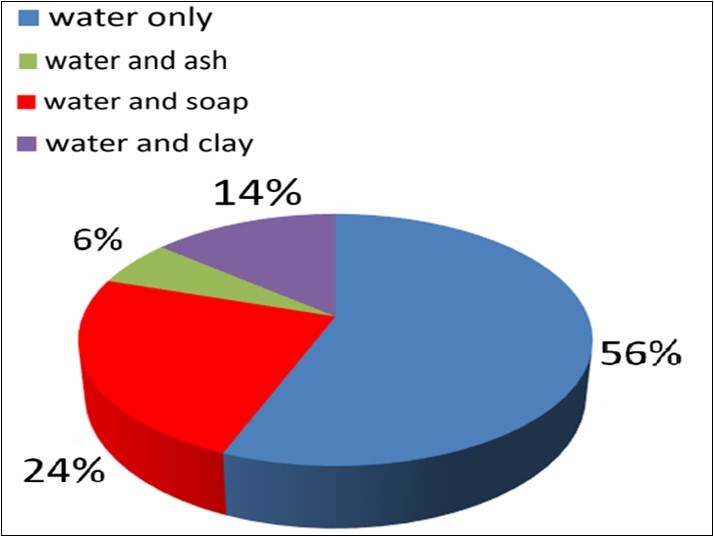
Figure 8.Hand washing time of respondent Lodha mothers.
The overall hand wash score (mean ± SD) of the respondent mothers was 3.17 ± 0.87, which fall under the low category. Almost 97.2% of them had the ‘low’ hand wash score, 2.8% of them had an ‘average’ hand wash score. The overall WaSH score (mean ± SD) of the respondent mothers was 6.55 ± 2.2, which lie in the moderate category.
The majority of the respondents took a bath every day, but cloths were not changed daily. Bathing every day was mostly hampered when they go for a whole day outside job or begging. Around, 17% of the respondent mothers reported cutting nails on a regular basis. Almost 94 % women responded that they had no appropriate material during menstruation. About 46.4% of mothers of them had the ‘low’ WaSH score and 53.6% of them had an ‘average’ and ‘good’ WaSH score. WaSH score had significantly correlated with the Kuppuswamy SES score (r=0.088**, p<0.01) and monthly family income (r=0.104**, p<0.01).
Boys wore comparatively more dirty clothes than girl children. Children wash their teeth at least once a day, usually (67%) without a toothbrush and paste. Around 91% of children had a habit of consuming raw vegetables / fruit, and just 13% of them used to wash them with water.
Bathing Shelters
Majority (86%) of the respondent mothers takes a bath in the open water point predominantly at the pond (Figure 9). Bathing shelter was almost unavailable. If pond becomes dry, they bath at public tube well, bore whole water sources or open well water point which remained contaminated with garbage, plastics.
Figure 9.Places take bath by respondent Lodha mothers.
Drying Rack
They don't have tables for drying household utensils after washing predominantly of water and ash only (45%) (Figure 10). This study also exhibits that about 59% do not have a good practice in handling household utensils. They dry them on the ground and do not wash them at all before taking food.
Figure 10.material use during washing utensil by respondent Lodha mothers.
Clothing Line
Only about a third (32%) of the entire population have clothing lines for drying clothes (Figure 11). The two third populations (68%) still do not care or use other hygienic methods of drying clothes.
Figure 11.procedure of drying cloths by respondent Lodha mothers.
Knowledge about Basic Nutrition, Hygiene
The overall knowledge related to nutritional status and WaSH score (mean ± SD) of the mother was 3.3, which falls under low category. The results of this study showed that 79.2% of them had low nutritional knowledge, 14.8% of them had average nutritional knowledge. But, only 6.0% of them had good knowledge about nutrition. Only, 8.1% of mother knows about ORS is an essential for diarrhea patient. They were unaware about the common causes of diarrhea (Figure 12).
Figure 12.knowledge on causes of diarrhea of respondent Lodha mothers.
Predictors of knowledge score and WaSH score were calculated by logistic regression analysis (Table 1). It was observed that the resident district (AOR=0.24; 95% CI=0.17-0.33), number of children (AOR=1.08; 95% CI=0.76-1.5), mother education (AOR=1.28; 95% CI=0.9-1.8), type of family (AOR=1.10; 95% CI= 0.79-1.8) and type of house (AOR=3; 95% CI=1.4-6.2) was the predictor of poor WaSH scores of the respondent. Whereas, the Kuppuswamy SES score (AOR=5.2; 95% CI=1.3-21.8) and mother education (AOR=53.7; 95% CI=31.9-90.1) was the predictor of the knowledge score. The study also found that there is a significant relationship between knowledge score and residence district (χ2=26.09; p<0.01), Kuppuswamy SES score (χ2= 38.8, p<0.01), mother education (χ2= 5.144; p<0.05).
Table 1. Logistic regression analysis of knowledge score and WaSH score with socioeconomic status of Lodha women.| Variables | Factors | Knowledge score | WaSH score | ||||||
| Poor% | Average & good % | COR (95% C.I) | AOR (95% C.I) | Poor% | Average & good % | COR(95% C.I) | AOR(95% C.I) | ||
| Number of Child | ≥2 child(n=698) | 20.4 | 5.4 | 1 | 1 | 13.2 | 12.7 | 1 | 1 |
| <2child(n=243) | 58.9 | 15.3 | 0.979 (.683-1.40) | 0.875 (.505-1.51) | 33.2 | 40.8 | 1.28(0.95-1.72) | 1.081(.76-1.5) | |
| Residence District | Paschim Medinipur(n=595) | 47.2 | 16 | 1 | 1 | 20.5 | 42.6 | 1 | 1 |
| Jhargram(n=346) | 32.1 | 4.7 | 0.42 (0.29-0.61) | 0.806 (.47-1.37) | 26 | 11 | 0.2 (0.15-0.27) | 0.24**(0.17-0.33) | |
| Age of women | <30 yrs.(n=753) | 72.6 | 20.2 | 1 | 1 | 41.1 | 51.6 | 1 | 1 |
| ≥30 yrs.(n=59) | 6 | 1.2 | 0.734 (0.364-1.48) | 0.744(.28-1.93) | 3.6 | 3.7 | 0.82(0.48-1.4) | 0.99(0.55-1.7) | |
| Kuppuswamy SES score | Lower (< 5)(n=901) | 78.1 | 19.9 | 1 | 1 | 45.5 | 52.6 | 1 | 1 |
| Upper-lower (≥5)(n=38) | 1.2 | 0.9 | 2.85 (1.13-7.18) | 5.180** (1.31-21.81) | 0.9 | 1.1 | 1.08(0.42-2.7) | 0.94(0.3-2.8) | |
| Education of mother | No formal education(n=709) | 71.9 | 3.4 | 1 | 1 | 37.7 | 37.9 | 1 | 1 |
| Literate(n=232) | 7.3 | 17.3 | 49.9 (31.7-78.5) | 53.7*** (31.95-90.07) | 8.8 | 15.6 | 1.76(1.3-2.4) | 1.28(0.9-1.8) | |
| Family type | Joint(n=315) | 28 | 5.6 | 1 | 1 | 14.6 | 19.2 | 1 | 1 |
| Nuclear(n=626) | 51.1 | 15.3 | 0.663 (0.46-0.94) | 0.417*** (.248-.703) | 31.5 | 34.8 | 1.19(0.9-1.57) | 1.1(0.79-1.5) | |
| House type | Kutcha(n=879) | 74.3 | 19.7 | 1 | 1 | 44.9 | 49.2 | 1 | 1 |
| Pukka(n=57) | 4.9 | 1.2 | 0.903 (0.459-1.77) | 1.318 (0.50-3.44) | 1.3 | 4.6 | 3.19(1.6-6.1) | 3.0**(1.4-6.2) | |
Practices During Pregnancy and Lactation
The stoppage of menstruation cycle (first sign of pregnancy) was not a major concern for childbearing mothers. The majority of Lodha mothers were aware of sterilization for birth control, but spacing methods of birth control were less known. Home delivery (54%) was the prevailing custom among the Lodha families surveyed. According to the antenatal report card of respondent mothers the prevalence of low birth weight baby was 49%. Exiling of the first colostrum (13%) after delivery has been reported especially home delivery cases. On the 21stday after successful delivery both mother and baby take a purificatory bath and pare nails. Preference for boy children exists in the families.
Morbidity
The morbidities related to WaSH among Lodha mothers and children were very high (Table 2). A diarrheal form of morbidity within the 15 days of the survey was 2.6% of the mother and 9.2% of the children. Mother with age higher than 30 years, the prevalence of diarrhea was lower as compared to aged ≤30 years (0.4% Vs. 2.2%). But in case of children, the prevalence of diarrhea was increased gradually (1st years- 0.4%, 2nd year-0.9%, 3rd year-1.9% , 4th year-2.7%, 5th year-2.3%) with age and it was statistically significant (χ2=21.34, p<0.01). Mothers usually consult with the local quack doctor when they become sick. Furthermore, they also had faith of their own traditional medicine.Prevalence of morbidity was decreased with increasing age of the mothers, but had no significant difference. Lodha children who were resident of Paschim Medinipur district had a higher risk to be suffering from diarrhea significantly (p<0.05). The children were susceptible to be suffering from diarrhea whose mother did not wash their hands properly and it was found statistically significant.
Table 2. Prevalence of diarrhea with the socioeconomic and WaSH factors among Lodha women (n=941) and children (n=1043) of West Bengal.| Variables | Factors | Mother’s diarrhea | Children’s diarrhea | ||
| Prevalence (%) | χ2 (Sig.) | Prevalence (%) | χ2(Sig.) | ||
| Mother education | No formal education(n=709) | 1.7 | 1.19(0.75) | 6.2 | 2.59(0.46) |
| Primary (n=228) | 0.9 | 2.8 | |||
| Secondary (n=3) | 0 | 0 | |||
| H.S (n=1) | 0 | 0 | |||
| House type | Kutcha (n=879) | 2.5 | 1.5(0.2) | 7.6 | 0.003(0.96) |
| Pukka (n=57) | 0.1 | 0.5 | |||
| Safe Drinking water | Available (n=328) | 1.2 | 2.4(0.1) | 3.3 | 2.46(0.17) |
| Not Available (n=613) | 1.2 | 5.4 | |||
| Latrine | No (n=914) | 2.6 | 0.5(0.4) | 8.8 | 1.7(0.19) |
| yes (n=27) | 0 | 0.4 | |||
| District of residence | Paschim Medinipur(n=595) | 1.2 | 3.2(0.07) | 6.9 | 7.9(P<0.05) |
| Jhargram(n=346) | 1.4 | 2 | |||
| Kuppuswamy SES | Lower (< 5) (n=901) | 2.4 | 0.48(0.5) | 8.9 | 1.9(0.17) |
| Upper-lower (>5) (n=36) | 0.2 | 0 | |||
| Family Member | <4 person (n=471) | 1.8 | 2.16(0.14) | 4.7 | 0.52(0.47) |
| >4person(=572) | 0.7 | 4.3 | |||
| WaSH Score | Low(n=428) | 1.8 | 5.8(P<0.05) | 3.4 | 2.71(0.09) |
| Average and high(n=493) | 0.8 | 5.5 | |||
| Knowledge score | Low(n=746) | 1.9 | 0.27(0.6) | 6.7 | 1.02(0.31) |
| Average and high(n=195) | 0.6 | 2.2 | |||
| Wash hand before food | No (n=917) | 1.8 | 1.8(0.18) | 7.0 | 5.13(P<0.05) |
| Yes (n=124) | 0.6 | 1.9 | |||
| Wash hand properly after defecation | No (n=918) | 2.3 | 6.9(0.009) | 8.6 | 0.44(0.83) |
| Yes (n=123) | 0.3 | 0.3 | |||
Logistic regression shows the respondent mother who had more than two children (AOR=1.1; 95% C.I=0.34-3.5), no formal education (AOR=2.23; 95% CI=0.59-8.34), takes unsafe drinking water (OR=6.9; C.I-0.34-3.5), resident of Paschim Medinipur district (AOR-3.4; 95% C.I=1.04-10.8), greater than four (> 4) family member (AOR=2.2; 95% C.I=0.78-6.4) was greater risk to be suffering from diarrhea.
Nutritional Status of Mother and Children
Almost 41.6% Lodha mothers were suffered from chronic energy deficiency (CED: BMI <18.5 kg/m2). The prevalence of overweight & obesity (BMI≥25 kg/m2) among Lodha women was 1.6%. Whereas, 48.9% women were undurnutrition based on MUAC less than 22.0 cm. Moreover, the overall prevalence of wasting, stunting and underweight among preschool Lodha children was 31.9%, 62.1% and 61.3%, respectively. The WaSH score of the family was significantly associated with children to be stunted and underweight. The WaSH score of mothers was significantly different (P<0.01) with the occurrence of undernutrition, normal and overweight individual (BMI cut-offs) and MUAC. But knowledge score had no significant effects on BMI (Table 3).
Table 3. Relationship between knowledge and WaSH score with the nutritional status of mothers and children of the Lodha community of West Bengal.| Variables | Factors | Knowledge score | WaSH score | Wash hand before food | Wash hand after defecation | ||||||||
| Low% | Moderate to high % | χ2 (Sig.) | Low % | Moderate to high % | χ2 (Sig.) | No% | Yes% | χ2 (Sig.) | No% | Yes% | χ2 (Sig.) | ||
| Mother nutritional status | |||||||||||||
| BMI | <18.5 kg/m2(n=390) | 33.0 | 8.6 | 0.32(0.9) | 15.1 | 26.1 | 24.0 (P<0.01) | 35.2 | 6.3 | 2.1(0.34) | 40.1 | 1.4 | 1.1(0.57) |
| 18.5-24.9 kg/m2(n=533) | 45.0 | 11.7 | 30.4 | 26.9 | 50.3 | 6.9 | 55.5 | 1.7 | |||||
| ≥25 kg/m2(n=15) | 1.2 | 0.4 | 0.8 | 0.7 | 1.1 | 0.2 | 1.2 | 0.1 | |||||
| MUAC | <22cm (n=455) | 39.9 | 9.0 | 2.9(0.08) | 20.2 | 28.5 | 9.06(p<0.01) | 41.9 | 7.1 | 1.7(0.18) | 47.9 | 1.1 | 3.03(0.08) |
| ≥22 cm (n=474) | 39.3 | 11.7 | 26.4 | 24.9 | 45.1 | 5.9 | 48.9 | 2.2 | |||||
| Children nutritional status | |||||||||||||
| Underweight | Yes(n=576) | 48.0 | 13.3 | 0.79(0.4) | 26.3 | 35 | 6.97 (P<0.05) | 50.4 | 8.8 | 10.1(p<0.01) | 3.1 | 54.1 | 25.1(P<0.01) |
| No(n=363) | 31.2 | 7.5 | 20.0 | 18.6 | 37.8 | 3.4 | 5.8 | 34.1 | |||||
| Stunting | Yes(n=583) | 48.6 | 13.5 | 0.96(0.3) | 25.2 | 36.6 | 18.15 (P<0.01) | 50.1 | 9.2 | 15.5(P<0.01) | 2.5 | 55.0 | 40.2(P<0.01) |
| No(n=356) | 30.7 | 7.2 | 21.1 | 17.1 | 37.8 | 3.0 | 6.4 | 33.2 | |||||
| Wasting | Yes(n=300) | 24.8 | 7.1 | 0.65(0.4) | 15.2 | 16.5 | 0.43(0.5) | 27.6 | 3.8 | 0.01(0.9) | 2.3 | 28.1 | 1.35(0.5) |
| No(n=639) | 54.4 | 13.6 | 31.1 | 37.1 | 60.2 | 8.4 | 6.6 | 60.1 | |||||
The Logistic regression analysis showed that the Lodha boys were 1.2 times greater risk to be suffering from underweight than girls. Mother with CED had 1.6 (P<0.05) and 1.5 (P<0.05) times more risk to be developed child stunting and underweight. Lack of safe drinking water was also an important predictor, as children were 1.7 (P<0.05) times and 1.6 (P<0.05) times higher risk to be developed stunting and underweight. More importantly, children were significantly 2.5 times and 1.2 times higher risk for stunting and underweight, whose mothers do not wash their hands properly after defecation. Moreover, the children were 1.6 times greater risk to be wasted, if the family had no sanitary latrine facilities.
Discussion
Maintaining healthy growth and development of child, safe drinking water, hygiene and sanitation play a significant role. So, present study carried out to investigate the sanitation and hygienic practices of Lodha mothers of Paschim Medinipur and Jhargram districts of West Bengal, are both drought and flood prone area. In this area surface water becomes dry during summer season. Their major source of drinking water among the study population was tube well, but fair section utilizes open well water for consumption. In general, they did not wash main drinking water preserver on a regular basis for making water safe to drink. The use of open buckets and pots without a lid was a poor practice. Additionally, the dipping method of fetching water from the storage container remained a predominant practice among the Lodha population, all may lead to contamination.
It was observed that the nutritional status of Lodha women and children was not satisfactory. According to the WHO, prevalence of wasting, stunting and underweight among preschool children was very high. The socioeconomic status, including literacy and income of this community was very low. Sanitation, hygienic practices and the maternal factors were the important predictors of the nutritional status of the children. The knowledge of the Lodha mother in Paschim Medinipur was very poor in terms of safe food, water and sanitation. This study found children of family with lack of safe drinking water was 1.7 and 1.6 times times higher risk to be developed stunting and underweight. A study from north-western Uganda, documented children with families used water from unprotected resources were more underweight than their counterparts 19. Another study report, the children become more risk to be underweight, if the water is used from the unprotected source than the safe source 20. In India, 46.6% of houses have the accessibility of drinking water within the premises, 35.8%, nearby the premises and 17.6% outside the premises 8. The Lodha women had to go for a long way to collect clean and safe drinking water during summer season. The most respondents wash their utensils and hands with water, clay or ash with water. It was established that parent’s education was correlated with substantially higher WaSH ratings. A community-based cross-sectional study conducted in the rural region of Kerala among 103 mothers of preschool children is probable to have changed water and hygiene practices due to the higher educational status of mothers 19. Our results showed, WaSH score was significantly different among stunted and underweight children.
Families having latrine add comfort and dignity to the household. Latrines also facilitate defecation practices any time of the day or season and it removes worry about insect or snake bites or feel embarrassed when guests come to visit. In our study, the majority (84.8%) of the adult members and 83.6% of their under-five children were practicing open field defecation, which increased the risk of waterborne diseases. The Lodha children were more wasted (1.6 times) due to non-availability of sanitary latrine facilities. According to the census 2011, in India, 53.1 % households had no latrine facilities within the premises and out of them, 49.8% does open defecation 8. Often, open defecation practices contribute to the high occurrence of diarrhea and other waterborne diseases.
This study found, after defecation water and soap was used by 24% participants. Our results were higher than that reported by a study, where 10.8 % went through soap to wash their hands before meals, and 19 % washed their hands after used toilet 20. In contrast, a study from the urban slums of West Bengal and Tripura reported that over 90% of the study population practiced hand washing after defecation 23. Our results were lower compared to a study conducted among 57 mothers in Indonesia, reported 43% of mothers used soap to wash their hands as well as their children's hands after defecation 24. The shortage of water has an effect on hand washing. Frequent and proper hand washing is one of the most efficient steps that can be used to avoid infection. A study documented, poor environmental sanitation and un-hygienic personal habits appear to influence to the recurrent infections of the children, which is associated with malnutrition 25.
Conclusion
Lodha is a particularly vulnerable tribe living in Paschim Medinpur and Jhargram districts of West Bengal with sustained poverty. A lion share of the respondents have to used water from an open well (contaminated sources) in the hot summer season. Since, other safe drinking water resources were not adequate. The Lodha population was significantly suffering from diarrhea and other waterborne diseases due to their faulty WaSH practices. There is good association between poor household WaSH practices with child undernutrition and morbidity. A significant proportion of these can be prevented by proper WaSH practices. Hence, there is urgent need to develop the comprehensive knowledge attitude and practice (KAP) guidelines in their language to educate them about appropriate water storage, retrieval methods, sanitation and hand washing practices.
Funding
None
References
- 1. (2014) WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation Progress on drinking water and sanitation. update. UNICEF: Annual Results Report. Water, sanitation, and hygiene
- 5.Hoque B A. (2003) Hand washing practices and challenges in Bangladesh. , Int J Environmental Health Res 13, 81-87.
- 6.World Health Organization. (2005) Flooding and communicable diseases fact sheet. Weekly Epidemiological Record= Relevé épidémiologique hebdomadaire. 80(03), 21-28.
- 7.Naghavi M, Abajobir A A, Abbafati C. (2007) Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study. , Lancet 390(10100), 1151-1210.
- 8.Census of India (2011) Census of India: Provisional Population Tables, Registrar General and Census Commissions of India. Government of India. , New Delhi, India
- 9.Dodos J, Mattern B, Lapegue J, Altmann M, Aissa M A. (2017) Relationship between water, sanitation, hygiene, and nutrition: What do Link NCA nutrition causal analyses say?. , Waterlines 36(4), 284-304.
- 10.Black R E, Victora C G, Walker S P. (2013) Maternal and child undernutrition and overweight in low-income and middle-income countries. , Lancet 382(9890), 427-451.
- 11.Victora C G, Adair L, Fall C. (2008) Maternal and child undernutrition: consequences for adult health and human capital. , Lancet 371(9609), 340-357.
- 12.Rah J H, Cronin A A, Badgaiyan B, Aguayo V, Coates S et al. (2015) Household sanitation and personal hygiene practices are associated with child stunting in rural India: a cross-sectional analysis of surveys. , BMJ 5(2), 005180.
- 13.GuruRaj M S, Shilpa S, Maheswaran R. (2015) Revised socio-economic status scale for urban and rural India – Revision for Socioeconomica. 4(7), 167-174.
- 14.Lohman T G, Roche A F, Martorell R. (1988) Anthropometric standardization reference manual. Chicago: Human Kinetics Books.
- 15.World Health Organization. (1995) Physical status: The use and interpretation of anthropometry. Technical Report Series No. 854. Geneva: WHO
- 16.WPT James, CGN Mascie-Taylor, Norgan N G, Bristrian B R, Shetty P et al. (1994) The value of arm circumference measurements in assessing chronic energy deficiency in Third World adults. , Eur J Clin Nutr 48, 883-894.
- 17. (2006) WHO Multicentre Growth Reference Study Group. Assessment of differences in linear growth among populations in the WHO Multicentre Growth Reference Study. Acta Paediatr. 450, 56-65.
- 18.Reddy B V, Kusuma Y S, Pandav C S, Goswami A K, Krishnan A. (2017) Water and sanitation hygiene practices for under-five children among households of Sugali tribe of Chittoor district. , Andhra Pradesh, India. J Environ Public Health. ID 7517414.
- 19.Vella V, Tomkins A, Borghesi G B, Mighori G B, Adriko B C et al. (1992) Determinants of child nutrition in North West Uganda. , Bull World Health Organ 70, 637-643.
- 20.Gamecha R, Demissie T, Gelaye A. (2017) The magnitude of nutritional underweight and associated factors among children Aged 6-59 months in Wonsho Woreda, Sidama Zone Southern Ethiopia. , Open Public Health J 10, 7-16.
- 21.Divya S, Saju C R, Navya C J, Joshy V M, Jini M P et al. (2016) A study on selected behavioral factors of mothers influencing acute diarrhoea in under- five children in a rural part of Kerala. , India. Int J Community Med Public Health 3, 2211-2216.
- 22. (2011) The HUNGAMA Survey Report. http://www.naandi.org/wp-content/uploads/2013/12/HUNGaMA-Survey-2011-The-Report.pdf
- 23.Ray S K, Zaman F A, Laskar N B. (2010) Hand washing practices in two communities of two states of Eastern India: an intervention study. , Indian J Public Health 54(3), 126-130.
Cited by (9)
This article has been cited by 9 scholarly works according to:
Citing Articles:
International Journal of Social Determinants of Health and Health Services (2025) Crossref
International Journal of Social Determinants of Health and Health Services (2025) OpenAlex
The Oriental Anthropologist: A Bi-annual International Journal of the Science of Man (2024) Crossref
The Oriental Anthropologist A Bi-annual International Journal of the Science of Man (2024) OpenAlex
(2023) OpenAlex
Journal of Water, Sanitation and Hygiene for Development (2023) Crossref
Journal of Water Sanitation and Hygiene for Development (2023) OpenAlex
Journal of Law and Sustainable Development (2023) Crossref
Journal of Law and Sustainable Development (2023) OpenAlex