
Influence of Education Sources on Osteoporosis Knowledge and Calcium Intake in Adult Women: A cross sectional Study
Abstract
Osteoporosis prevention among women requires obtaining proper knowledge early in life about the disease, risk factors and treatments. This study compares specific education sources to osteoporosis knowledge and calcium intake. Online survey usinga convenience sampling was performed with women between ages 18 and 40. The survey measured osteoporosis knowledge, calcium consumption, and specific education source within categories of age, school classes, television, radio, newspaper, magazine, Internet, and in-person. Multiple regression analysis determined influential education sources for osteoporosis knowledge and calcium intakes. Osteoporosis knowledge was suboptimal (13.8 ± 3.3, as a score higher than 16 defined as “adequate”) and average daily calcium intake was 1315.1 ± 609.9 mg. Age and newspaper had greatest contribution towards osteoporosis knowledge, while Internet, school classes and radio were most influential resources on calcium intakes. Creating an osteoporosis education initiative utilizing these sources is imperative for increasing disease knowledge and preventive behavior among young women.
Author Contributions
Academic Editor: Marcello Iriti, Milan State University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2014 Amanda Unanski Enright, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Osteoporosis is a silent epidemic among postmenopausal women and the elderly worldwide.1, 2 The Surgeon General identified 10 million Americans over the age of 50 with osteoporosis, 34 million at risk, and predicted half of women over the age of 50 will have an osteoporotic fracture in their lifetime.3 Reduced bone density can be the result of inadequate growth and/or excessive loss of bone tissue, all of which increase the likelihood of fracture.4 To ensure a slow rate of bone tissue deterioration after age 30, maximum peak bone mass must be accumulated from childhood through early adulthood.5 Peak bone mass accumulation is the result of interactions between internal factors, including hereditary and hormonal, and external factors, including nutrition and physical activity.4 Physical activity, and in particular weight-bearing exercise, has demonstrated benefits before and after puberty in areas such as the hips, wrists, and legs.6, 7
One goal of Healthy People 2020 is to reduce osteoporosis among adults aged 50 and over by 10%, although prevention against the disease begins well before women enter this age bracket.8, 9 Consuming an appropriate diet of calcium and vitamin D, along with performing weight-bearing exercise, is within control of the individual, yet there is a lack of preventive behavior during the adolescent and young adult years when building peak bone mass is crucial9, 10. Knowledge and attitude about osteoporosis, prevention, and treatment have been examined to identify where the gap exists in moving towards preventive behavior, yet an ideal solution is still outstanding1, 11, 12.
Osteoporosis knowledge has been linked to preventive behavior among young adult as well as post-menopausal aged females.1, 13, 14, 15 Top sources of osteoporosis knowledge among multiple female populations include media, Internet, relatives, health professionals, and materials available at healthcare offices.16, 17, 18 Despite the various sources available providing osteoporosis information to women of various ages, studies have shown that knowledge levels about the disease are consistently low.16, 17, 18, 19, 20
Calcium intake among women in the United States has also been inadequate. Many women ages 19-50 do not meet the Recommended Dietary Allowances (RDA) of 1,000 mg/day, despite using calcium supplements.21, 22 Diets consisting of unprocessed dairy products, protein, fruits and vegetables low in salt contribute to a bone-healthy diet and increased bone mineral density, as high amounts of salt in the blood reduces calcium retention in the bones and causes calcium loss in urine.11 Many adolescents and young women are unaware of foods that offer high sources of calcium beyond dairy products.23
The ideal time to educate women about osteoporosis and bone health is during childhood and adolescence23. Divergent sources of bone health and calcium may provide conflicting information resulting in low levels of knowledge about the disease. This low level of knowledge in turn negatively impacts osteoporosis preventive behavior, such as calcium intake. In order to determine an optimal intervention strategy for reducing instances of osteoporosis, the objectives of this study are to determine osteoporosis knowledge and current calcium intake among adult, premenopausal women, while determining originating sources of knowledge to overall disease comprehension and actual calcium intake.
Materials and Methods
The questions this study aims to answer are: the current level of osteoporosis knowledge among adult women; the average daily calcium intake among adult women; the primary sources from which adult women have obtained knowledge about osteoporosis; the way these sources compare to both knowledge level and calcium intake.
A cross-sectional survey was conducted with women ages18-40 during spring 2012. This age range was utilized to obtain input from the premenopausal adult female population. Women typically begin to enter menopause after age 40; this study did not include women above this age, as it has been found women of menopausal age have greater awareness about osteoporosis and are actively seeking information, in addition receiving more education from their healthcare providers during this timeframe.20 Convenience sampling methods were used to recruit participants via email, social media websites. Sample size was determined using power calculation24: minimum sample of 226 based on the number of survey variables that would achieve 80% power at a significance level of 0.05. Fliers were posted around campus at two universities and a gym in central New Jersey. All recruitment methods included a link to the survey that the participants accessed. An incentive was offered to potential participants for entry into a gift card raffle. The Institutional Review Board at one university in New Jersey approved the study protocol. All eligible participants received a consent form detailing the purpose and procedure of the study. Participants could not begin the survey until consent was given, and could withdraw from the survey at any time.
The survey measured osteoporosis knowledge, average daily calcium intake, and identified sources of osteoporosis education using validated instruments, Facts on Osteoporosis Knowledge Quiz and Short Calcium Questionnaire.20, 25
Osteoporosis Knowledge and Calcium Intake
The Facts on Osteoporosis Knowledge Quiz is a 20-question true/false knowledge test based on the National Institutes of Health Consensus Report on osteoporosis20. Study participants were unable to change their responses once the knowledge test was submitted. The participants did not receive a copy of their knowledge score, nor were they provided with answers to the questions upon completion to help maintain the integrity of the study.
On the Short Calcium Questionnaire, each participant reported weekly intake of specific foods, such as milk, cheese, legumes, and calcium-fortified products. In addition, participants identified any supplements taken that may contain calcium, including multi-vitamin/mineral supplements, and antacids along with the amount of calcium in milligrams each supplement contains. The participants’ daily average calcium intake was then compared to the RDA for adult females.21
Education Sources
A tool specifically designed for this study was used for participants to identify their sources of osteoporosis education. The 8-question tool asked participants to identify sources from the following categories:1) Age (e.g. elementary, secondary, college, post-graduate);2) Specific Classes (e.g. elementary-level health class, high school biology, college-level nutrition class);3) Television (e.g. news program, television talk show); 4) Radio (e.g. AM radio, FM radio, satellite radio); 5) Newspaper (e.g. national newspaper, local newspaper); 6) Magazines (e.g. women’s health, beauty, fitness); 7) Internet (e.g. medical website, search engine, online news site); 8) In-person (e.g. primary care physician, OB/GYN, family member, friend).
Analysis
All data were collected using the online survey and each participant was assigned a random identification number. Individual knowledge scores were calculated following the instrument guidelines: each correct answer receiving one point, and zero point for each incorrect or “don’t know” answer, up to a total of 20 points20. Calcium intake was calculated using the formula provided in the instrument, which determined an average daily calcium intake compared to RDA24.
Multiple regression analysis was used to determine influential osteoporosis education sources on knowledge level and calcium intake. Each category (age, class, television, radio, newspaper, magazine, internet, and in-person) was analyzed through comparison of the specific education sources to the knowledge scores of the sample. For example, the four sources of the ‘age’ category were entered to the regression model that has ‘knowledge scores’ as the dependent variable. Two sources of the ‘newspaper’ category were regressed on the ‘knowledge scores.’ This method of model fitting was performed for each knowledge category, to find significant sources for the knowledge scores. For calcium intake, all sources of each category were again regressed on the ‘calcium intake,’ in order to determine the influential sources for calcium intake. In addition, the association between the knowledge score and calcium intake was examined using a correlation technique (Pearson’s r, correlation coefficient). Statistical Package for the Social Sciences (SPSS) Version 20.0 was used for analysis. The criterion of significance for the multiple regression models, and correlation was set at 0.05.
Results
A total of 228 participants completed the survey. The mean age of participants was 28.7 years (SD 4.4). They were primarily white Caucasian (89%), highly educated (70% above bachelor’s degree), and engaged in regular exercises more than 3 times/week (77.2%). The mean knowledge score was 13.8 (SD 3.3). A score of 16 or higher on the osteoporosis knowledge indicates adequate knowledge; 79 respondents (34.6%) earned scores of 16 or above. Questions with the highest frequency of correct responses were: “Normally, bone loss speeds up after menopause” (91.2% correct), “A lifetime of low intake of calcium and vitamin D does not increase the risk of osteoporosis” (90.4% correct) and “Physical activity increases the risk of osteoporosis” (89.0% correct), while the lowest incidence of correct responses was for: “Walking has a great effect on bone health” (4.8% correct) and “Low weight women have osteoporosis more than heavy women” (34.6% correct). Questions that received the lowest number of correct scores also had a high incidence of “don’t know” responses.
Based on the responses provided in the calcium questionnaire, the sample population had a mean daily average calcium intake of 1315.1 mg (SD 609.9). Top dietary sources of calcium for the participants were cheese, milk, and broccoli/collards/kale. Over half respondents take a multi-vitamin/mineral supplement containing calcium. Within the sample population, 36% were inadequately meeting the RDA for calcium, while 5% actually had excessive intakes over the upper limit of 2500 mg per day.
Figure 1 shows the educational sources identified by the respondents. While specific education sources were identified in each category, there is also a majority of respondents who indicated they did not learn at all from certain categories. The most frequently named categories were in-person, television, age and school classes. High school-level education, family members, women’s health magazines, and high school-level health class were the most frequently named specific sources of osteoporosis education.
Figure 1.Educational sources of osteoporosis knowledge (N=28)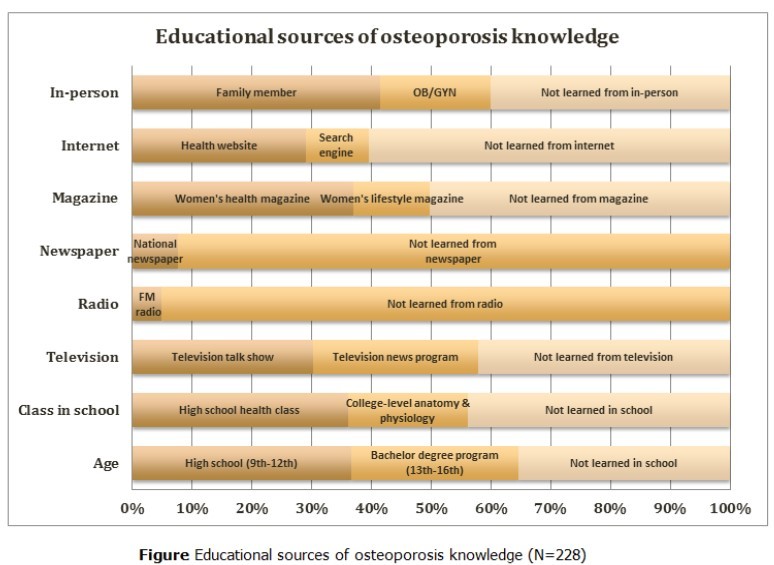
Educational Sources Compared to Knowledge Score and Calcium Intake
A correlation analysis of knowledge to calcium intake found weak and non-significant relationship (r=0.12, p=0.6). Multiple regression analysis determined influential sources on knowledge scores and calcium intake. Age, class in school, and Internet were source categories that contributed to osteoporosis knowledge as shown in Table 1. Within the age category, graduate degree level (b=0.16; p=0.01) and doctorate degree (b=0.13; p=0.03) were most influential on the knowledge score. A college-level anatomy & physiology class (b=0.11; p=0.01) was influential in the grade category, while health websites (b=0.15; p=0.03) were influential in the Internet category.
For calcium intake, school classes and Internet were most influential. A college-level anatomy & physiology class (b=0.18; p=0.01), health website (b=0.15; p=0.02), and government website (b=0.21; p=0.004) were the sources within these categories found to have the highest influence on calcium intake (Table 1).
Table 1. Significant Educational Sources for Knowledge and Calcium Intake| Sources | Knowledge Scores | Calcium Intake | |||
| Category | Sources | β | P | β | P |
| Age | College degree | 0.16 | 0.01 | Not significant | |
| Doctoral degree | 0.13 | 0.03 | |||
| School Class | College anatomy & physiology | 0.11 | 0.01 | 0.18 | 0.01 |
| Internet | Health website | 0.15 | 0.03 | 0.15 | 0.02 |
| Government website | Not significant | 0.21 | 0.004 | ||
Discussion
The knowledge level of the population sample was deemed inadequate, similar to prior studies of osteoporosis knowledge levels in the female population, ranging from adolescence to menopause.16, 17, 18, 19, 20 Knowledge and calcium intake was also found to be weakly associated, indicating that disease knowledge has little influence and calcium intake. The low knowledge level of the population justifies the need for more osteoporosis education targeted to young adult women, especially in the areas of risk factor, prevention, and treatment.
The average calcium intake of the sample population exceeds the RDA of 1,000 mg for women ages 19-40.21 The average may have been skewed due to 5% of the study population consuming excess calcium over 2,500 mg per day. This is contradictory to other studies that have been conducted to measure calcium intake in a female population utilizing calcium questionnaires, where average daily calcium intake was below the RDA.22, 26 Non-dietary of sources of calcium were obtained primarily through multi-vitamin/mineral sources, which range in calcium from 100 mg to over 1,000 mg per dose. Those taking high doses of calcium supplements display a knowledge gap in calcium absorption; the higher the amount of calcium that is ingested at once, the lower the bioavailability.27, 28 A maximum dose of 500 mg of calcium can be absorbed at one time, while undigested calcium can lead to the development of kidney stones and colon cancer, among other complications.21, 27 The identification of high calcium intake levels among the sample populations identifies a need to educate young women about calcium sources, appropriate RDA and UL (tolerable upper intakes) levels, and proper supplement dosing.
Although no one source of osteoporosis education was found to be an “ideal” source that would yield a higher knowledge score, it is important to note the higher calcium intake that occurred in this sample population as a result of obtaining information via Internet sources, especially health-related websites. One explanation may be that the Internet is a proactive source of information, in which the user may already have an interest in a topic they are researching and a desire to apply to daily life.29, 30 The finding of Internet usage’s influence on osteoporosis knowledge and calcium intake presents the opportunity to further explore education through online media channels.
Limitations of this study include recall bias and a lack of diversity in the sample population. Asking participants to identify learning about osteoporosis at a specific point in time, relied heavily on memory recall. Although the topic may have been touched upon at a certain point in their lifetime, there is a chance not all participants remember. Therefore conducting this study with adolescents may alleviate recall bias. The sample population also lacked racial and educational diversity, which can be addressed in future studies by expanding the recruitment initiatives beyond college campuses and recruit participants from both urban and suburban areas. Preliminary focus groups with representatives of the target population could help create a comprehensive source list of knowledge information sources.
Conclusion
While this study focused on adult women between the ages of 18-40, there is an opportunity to conduct a similar study among adolescent females in middle and high schools and compare the two populations. The adolescent women may also provide “real-time” learning about which osteoporosis information and knowledge sources they have been exposed to at this point in their lives, as opposed to the adult population, which relied heavily on memory recall.
The significance that Internet education sources had on calcium intake opens a future research opportunity about the effects of learning about osteoporosis online versus a traditional classroom setting and determine if knowledge outcomes and calcium intake is impacted by the educational approach. When taking into consideration the low knowledge scores of the study population, the Internet may be a viable option for increasing awareness by creating a public health campaign that incorporates online media into the program; this would allow individuals to interact more deeply with the content. It also eliminates the need to wait for a health care provider to bring up the topic of osteoporosis during an office visit, which typically is not broached unless the woman is nearing menopausal age or has experienced a related health issue, such as an eating disorder, that could impact her bone mineral density at an early age.31
References
- 1.M F Chan, W S Kwong, Zang Y, P Y Wan.Evaluation of an osteoporosis prevention education programme for young adults.J. AdvNurs.2007;57: 270-285.
- 2.A M Boot, Ridder M A J de, Sluis I M van der.Peak bone mineral density, lean body mass and fractures.Bone. 2010, 336-341.
- 3.US Department (2004) of Health and Human Services. Bone health and osteoporosis: A report of the Surgeon General. U.S. Department of Health and Human Services, Office of the Surgeon General Retrieved from http://www.surgeongeneral.gov/library/reports/bonehealth/content.htm , Rockville, MD: .
- 4.Matkovic V, Jelic T, G M Wardlaw.Timing of peak bone mass in Caucasian females and its implication for the prevention of osteoporosis.Inference from a cross-sectional model.JClinInvest.1994;93:. 799-808.
- 5. (2010) . Blake, J.S., Munoz, K.D., and Volpe, S. Major Minerals. In: Lindelof, S., Cechvala, C. eds.NutritionFromScience to You. 1sted. San Francisco, CA: Benjamin Cummings; 474-475.
- 6.C T, Tao C.Nature or nurture: Determinants of peak bone mass in females.JPediatrEndocrinolMetab. 2002, 1387-1393.
- 7.D L Nichols, C F Sanborn, E V.Bone density and young athletic women: An update.Sports Med. 2007, 1001-1014.
- 8.Department U S. (2020) Healthy and Human Services. Healthy People. http://www.healthypeople.gov/2020/topicsobjectives2020 Accessed .
- 9.C M Weaver.The growing years and prevention of osteoporosis in later life.ProcNutrSoc.2000;59:. 303-306.
- 11.M R French, Vernace-Inserra F, G A Hawker.A prospective study to identify factors affecting adherence to recommended daily calcium intake in women with low bone mineral density.J Am CollNutr.2008;27:. 88-95.
- 12.Bohaty K, Rocole H, Wehling K, Waltman N.Testing the effectiveness of an educational intervention to increase dietary intake of calcium and vitamin D in young adult women.J AmAcadNursePract. 2008, 93-99.
- 13.Berarducci A.Osteoporosis education: A health-promotion mandate for nurses.OrthopNurs.2004;23:. 118-120.
- 14.C A Sedlak, M O Doheny, S L Jones.Osteoporosis prevention in young women.OrthopNurs.1998;17:. 53-60.
- 15.L, Lynch J, T R Sullivan, J D McNeill.Osteoporosis education improves osteoporosis knowledge and dietary calcium: comparison of a 4 week and a one-session education course.IntJ Rheum. Dis.2011;14: 239-247.
- 16.Attia Al, M Abu, A, M.How much do the Arab females know about osteoporosis? The scope and the sources of knowledge.ClinRheumatol.2008;27:. 1167-1170.
- 17.Gemalmaz A, Oge A.Knowledge and awareness about osteoporosis and its related factors among rural Turkish women.ClinRheumatol.2008;27:. 723-728.
- 18.A, A J Shelton, T C Douglas, N J Rianon.Osteoporosis among perimenopausal African-American women: The relationship between sources of information and levels of knowledge about osteoporosis.J Natl Black Nurses Assoc. 2004, 40-47.
- 19.M J Kasper, Peterson M G E, J P Allegrante. (2001) The need for comprehensive educational osteoporosis prevention programs for young women: Results from a second osteoporosis prevention survey.Arthritis Care Res. 45, 28-34.
- 20.R L Ailinger, Braun M, Lasus H, Whitt K.Factors influencing osteoporosis knowledge: community study.J Community HealthNurs. 2005, 135-142.
- 21. (2014) Office of Dietary Supplements. Dietary supplement fact sheet:. , Calcium. http://ods.od.nih.gov/factsheets/Calcium-HealthProfessional. Accessed
- 22.K M Mangano, S J Walsh, K L Insogna, A M Kenny, J E Kerstetter.Calcium intake in the United States from dietary and supplemental sources across adults age groups:. New estimates from the National Health and Nutrition Examination Survey 2003-2006.J Am Diet Assoc 2011, 687-695.
- 23.J T Martin, C P, Gendler P.Female adolescents’ knowledge of bone health promotion behaviors and osteoporosis risk factors.OrthopNurs. 2004, 235-244.
- 24.D S Soper. (2014) A-priori sample size calculator for multiple regression (online software). http://www.danielsoper.com/statcalc3 Accessed .
- 25.N G Sebring, B I Denkinger, C M Menzie.Validation of three food frequency questionnaires to assess dietary calcium intake in adults.J Am Diet Assoc.2007;107:. 752-759.
- 26.Hacker-Thompson A, T P Robertson, D E Sellmeyer.Validation of two food frequency questionnaires for dietary calcium assessment.J Am Diet Assoc.2009;109:. 1237-1240.
- 27.R P Heaney.Factors influencing the measurement of bioavailability, taking calcium as a model.JNutr.2001;131: 1344S-1348S.
- 28.E A Yetley.Multivitamin and multimineral dietary supplements: definitions, characterization, bioavailability, and drug interactions.Am JClinNutr. 2007-85.
- 29.R J Cline, K M Haynes.Consumer health information seeking on the Internet – the state of the art.HealthEducRes. 2001, 671-692.
Cited by (2)
This article has been cited by 2 scholarly works according to:
Citing Articles:
International Journal Of Nutrition (2015) OpenAlex
International Journal Of Nutrition (2015) OpenAlex