
A Comparative Evaluation of the Role of Cone Beam Computed Tomography (CBCT) Imaging and Orthopantomography (OPG) in Sinus Augmentation Procedures: An Original Study
Abstract
Context:
The present study was undertaken to do a comparative evaluation of the role of Cone Beam Computed Tomography (CBCT) imaging and Orthopantomography (OPG) for pre-operative implant planning in combination with sinus grafting procedures in order to assess sinus anatomy and morphology and the existing bone height in three dimensions.
Aims:
To assess sinus anatomy and morphology and the existing bone height in three dimensions.
Materials and Methods:
Pre-operative assessment of maxillary sinuses for implant planning using CBCT imaging was performed on 20 sinuses (17 patients). These patients were subjected to orthopantomographs and CBCT imaging both pre-operatively and post-operatively. CBCT imaging helped to decide the type of sinus augmentation procedure best suited for the patients as per the individual needs and depending on the residual alveolar bone height, timing of implant placement, sinus morphology, anticipation of complication and comparative analysis between pre-and post-procedural gain in vertical alveolar bone height and increase in bone density.
Statistical Analysis:
The results were tabulated and statistically analyzed using Paired and Unpaired t-tests.
Results:
In the majority of cases, there was a concordance between the treatment type based on pre-operative and post-operative CBCT scans. The assessment of sinus morphology revealed a significantly higher detection rate of abberations in the form of sinus mucosal hypertrophy and septae on CBCT which were imperceptible on routine radiographs. The most appealing result was that vertical alveolar bone height could be measured precisely and there was a significant increase in surgical confidence and a significantly better prediction of complications when using CBCT imaging.
Conclusions:
A pre-operative planning based on CBCT imaging seems to improve sinus diagnostics and helps to execute a better treatment plan. Also, it is a good tool for the comparison of vertical alveolar bone height pre-and post-operatively following sinus augmentation procedures using various graft materials.
Author Contributions
Academic Editor: Allauddin Siddiqi, Sir Johan Walsh Research Institute, University of Otago
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 S.Girish Rao, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Apart from clinical evaluation, diagnostic imaging is an integral part of dental implant therapy for pre-operative planning and peri-and post-operative evaluations by use of various imaging techniques. Intra-oral radiography, although easily available and relatively inexpensive, is not considered satisfactory in giving reliable information regarding the anatomy of the region due to its major constraints of overlapping and superimpositions and geometric and anatomic limitations in the form of the measurements, for the teeth and surrounding bone and other anatomic landmarks, which change with a change in the angulations used during the exposure of the radiographs. Moreso, their being with, considerate overlapping and superimpositions, which is an inherent and practically impossible disadvantage to exclude, make them a little less reliable for planning implant therapy. For instance, extraoral radiography can be used and proven helpful in certain conditions in dentistry. With regard to orthopantomography, lack of image sharpness and resolution, apart from unequal magnification and geometric distortion, which are the major constraints in panoramic radiography, the other name for orthopantomography, often lead to an inaccurate interpretation and measurements.1 Although Computed Tomography (CT) is superior as it gives three dimensional, multi-planar reformatted images, with no superimposition of anatomic structures and with a high contrast and resolution, it is less acceptable owing to its leading to a relatively higher radiation exposure, cost, huge footprint and difficulty in accessibility. Hence, Cone Beam Computed Tomography (CBCT) was developed with distinct advantages in the form of reasonably low levels of radiation, the major drawback of CT, in addition to be able to provide a higher resolution that the conventional CT. CBCT uses a round or rectangular, cone shaped x-ray beam centred on a two dimensional x-ray sensor to scan a 360 degrees rotation around the patient's head. During the scan, a series of 360 exposures or projections, one for each degree of rotation, is acquired which provides the raw data for the final image re-construction with the help of computer software. Multiplanar reformatting of the primary reconstruction allows for both three and two dimensional images in any selected plane required. Also, CBCT has shown to be authentic and a good indicator of regenerated bone, pre-and post-procedures, for easy comparisons.1, 2 Currently, CBCT is being used for a number of applications in dentistry and suggested a useful diagnostic tool. In addition, various studies have concluded that CBCT imaging should be recommended for planning sinus augmentation procedures,3
however, there is a dearth of studies regarding the comparison between CBCT and panoramic radiography for planning sinus augmentation procedures prior to implant placement in the literature. The present study was undertaken to do a comparative evaluation of the role of Cone Beam Computed Tomography (CBCT) imaging and Orthopantomography (OPG) for pre-operative implant planning in combination with sinus grafting procedures in order to assess sinus anatomy and morphology and the existing bone height in three dimensions.
Materials and Methods
Sinus augmentation procedures were carried-out in 17 patients seeking implant options for oral rehabilitation including 10 for direct and 10 of indirect procedures (n=20, 10 direct and 10 indirect). The study comprised of 43% females and 57% males with a mean age of 46.07 years. A total of 17 patients (20 segments) satisfying the above criteria requiring placement of implants in atrophic maxilla/ increased pneumatisation of the maxillary sinus were selected for the study. The patients were informed about the study including the use of the synthetic graft material and their approval was sought before their inclusion in the study. A written informed consent was obtained from each of the participating patients. For each patient, a detailed case history was taken including chief complaint, history of presenting illness and medical history and personal history. A thorough clinical examination, including systemic and regional examination, was done. Patients with sinus pathology, previous sinus surgeries, chronic smokers, patients under 18 years of age, and with underlying systemic conditions which contradicts any surgical procedures were excluded from the study. The type of sinus lift was decided based on the pre-operative residual bone height evaluated radiographically. The residual bone height was recorded using CBCT scan and a computer based software where the measurements were made from the crest of the ridge till the sinus floor lining. Indirect sinus augmentation was done in patients with a bone height of <9mm but more than or equal to 5mm. Patients with a bone height of less than 5mm were taken up for direct sinus augmentation. The period of edentulousness varied from 6 months to 12 months. Apically tapered, commercially pure titanium implants (Life Care Devices Private Limited Mahim, West Mumbai, India) were used for patients undergoing indirect sinus augmentation. The length of implant was 8, 10, and 11.5 with diameters of 3.5, 4.0, and 5 mm respectively. Patients in the category of direct augmentation underwent the lateral approach procedure and augmentation with an alloplastic graft material. Implant placement was done after 6 months as the second stage procedure. The patients were assessed clinically at immediate post-operatively, and at 1 week, 1 month, 3 months, and 6 months post-operatively. Radiographic assessment for bone height was done pre-operatively and at 6 months post-operatively using cone beam computer tomography. In this comparative study, the measurements were tabulated and statistically analyzed to evaluate the difference in increase in bone height between direct and indirect sinus augmentation procedures radiographically. Orthopantomographs (screening tool) were taken to rule-out other pathologies and as a part of initial assessment. CBCT scans were assessed for pre-operative and post-operative bone height, bone width and bone density. The CBCT scans were obtained from Kodak 9300 which is a hybrid machine using a CS3D imaging software and flap panel detector sensor with exposure parameters of 90 KVp and 10 mA and resolution of 90 microns. The cross sections were made 1mm apart. (Image 1, Image 2, Image 3) The bone height measured pre-operatively using CBCT considered the pre-operative bone height as a measurement taken from the crest of the ridge till the sinus floor and post-operatively, from the crest till hyper-density evident apically. These measurements were standardized as a computer software drawing tool was used. Bone width was taken as the bucco-palatal width at three intervals- at the crest, 3mm from the crest and 6mm from the crest. Bone density was assessed visually by the width of trabecular pattern and were classified based on Misch‘s classification.4 Another additional bone density tool used was the pixel values (the gray scale values) obtained on the CBCT scan, although not reliable, and comparison done pre-operatively and post-operatively. The pixel values contained were a mean of three measurements obtained along the residual bone corresponding with the bone width levels.
Image 1.Routine sequential CBCT scans A and B) Axial sections; C) Cross section; D) Oblique sagittal section; E) 3-D reconstruction; F) Width measurement
Image 2.Axial section of CBCT showing sinus septae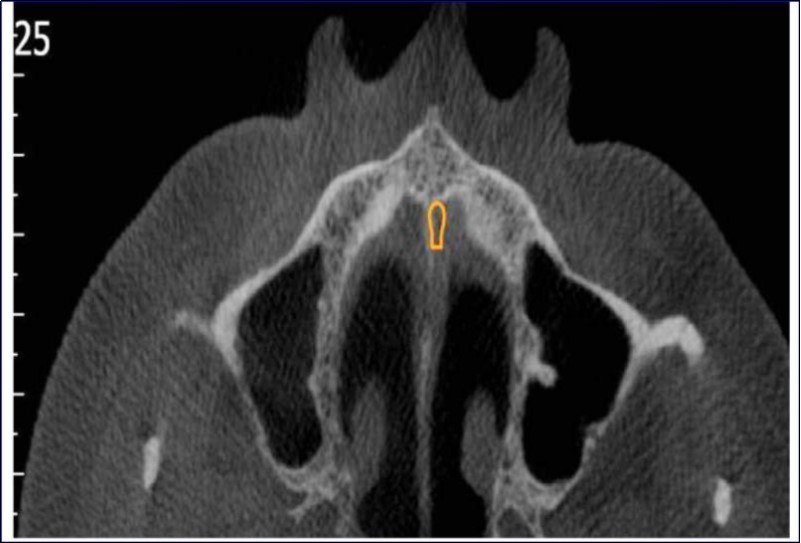
Image 3.Axial sections of CBCT showing sinus mucosal thickening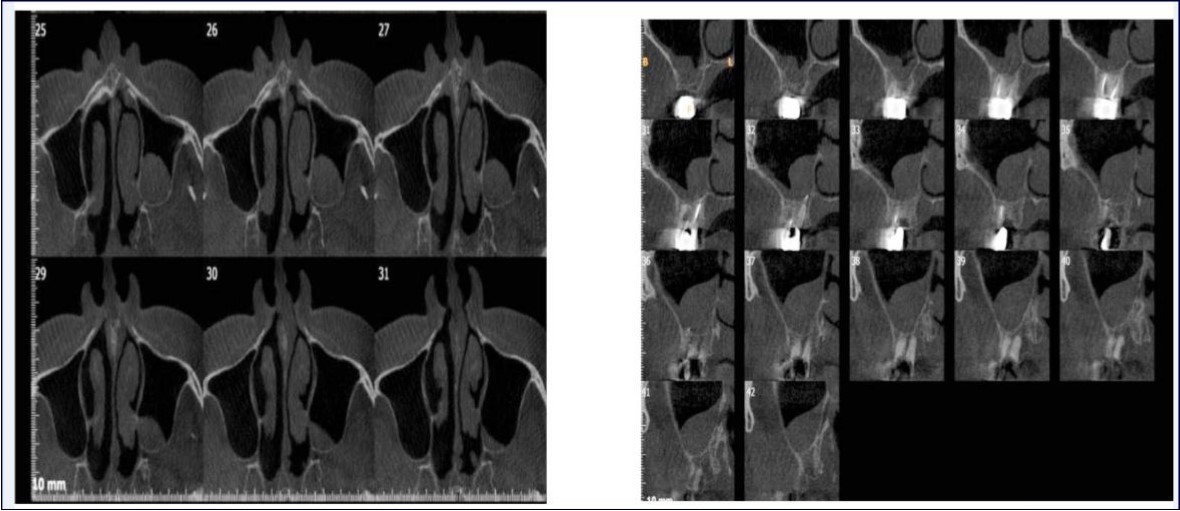
Statistical Analysis
The results were tabulated and the statistical analysis was carried-out. The statistical tests used for the analysis of the results were: Paired t-test; and Unpaired t-test.
Cases done with pre-operative CBCT evaluations (only 4 representative cases are being discussed to avoid repetition):
Case Report
With a pre-operative residual bone height of 0.8 mm in 16 region and 1.5 mm in 17 region, direct sinus augmentation was carried-out in a 40 year old male patient followed by implant placement of 3.75 x 11.5 dimensions as a single step procedure. Lateral window was created and synthetic graft material was dispensed through the lateral osteotomy site to maintain the elevated sinus membrane followed by placement of two dental implants through the crestal approach measuring 3.75 x 11.5 mm under local anesthesia and strict aseptic protocols. At the end of 6 months, a CBCT scan was advised to evaluate the increase in bone height which was 11 mm and 10.8 mm in 16 and 17 region respectively. (Figure 1, Figure 2)
Figure 1.Pre-operative Orthopantomograph and cross sections of CBCT showing residual alveolar bone height
Figure 2.Post-operative Orthopantomograph and cross sections of CBCT showing an increase in residual alveolar bone height
Case Report 2
A 45 year old patient with a residual bone height of 6.6 mm in 17 region underwent procedure of indirect sinus elevation using sinus osteotomy in relation to 17 region. Synthetic graft material was dispensed through the crestal osteotomy site to maintain the elevated sinus membrane followed by placement of a dental implant measuring 5 mm x 10 mm under local anesthesia and strict aseptic protocols. The implant was allowed to osseo-integrate for a period of six months during which the patient was followed periodically and was assessed for peri-implantitis, crestal bone loss and mobility. At the end of 6 months, a CBCT scan was advised to evaluate the increase in bone height which was 12mm. (Figure 3, Figure 4)
Figure 3.Pre-operative Orthopantomograph and cross section of CBCT showing residual alveolar bone height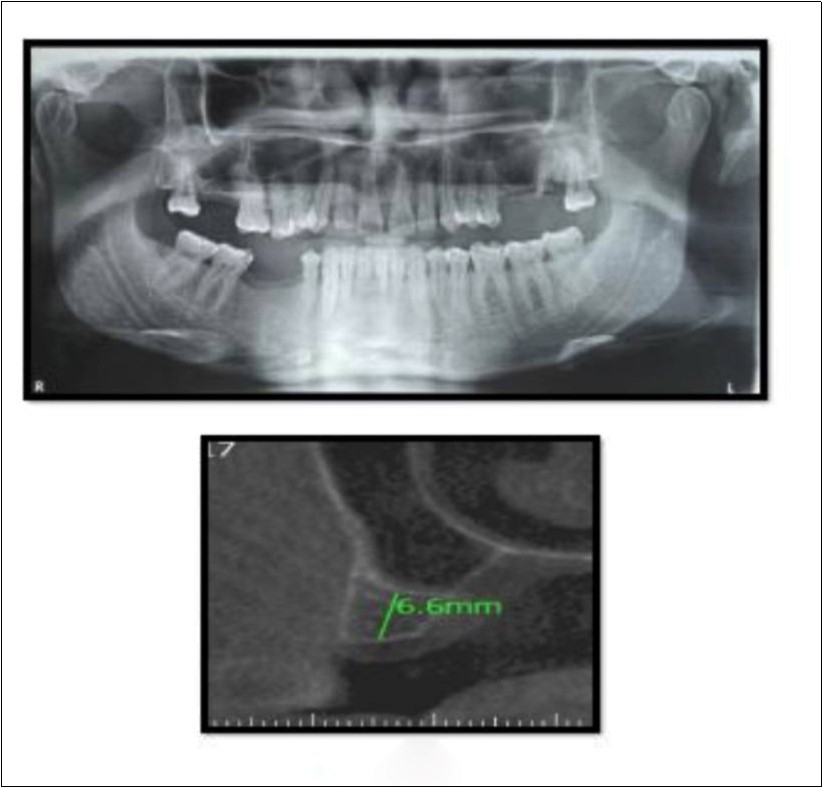
Figure 4.Post-operative Orthopantomograph and cross section of CBCT showing residual alveolar bone height
Case Report 3
A 75 year old man reported to the unit seeking options for replacement of his missing upper right first molar with fixed prosthesis. Due to the residual bone height of 5.3 mm, the patient was advised and subsequently, underwent the procedure of indirect sinus elevation using sinus osteotomy in relation to 16 region followed by placement of a dental implant measuring 5 mm x 10 mm under local anesthesia and strict aseptic protocols. The implant was allowed to osseo-integrate for a period of six months during which the patient was followed periodically. At the end of 6 months, a CBCT scan showed an increase in bone height to 11.5 mm. (Figure 5)
Figure 5.Pre-operative and post-operative Orthopantomographs and cross sections of CBCT showing residual alveolar bone height
Case Report 4
A 19 year old young woman was referred to Department seeking options for rehabilitation of missing right upper first molar with fixed prosthesis as she was uncomfortable with the removable partial denture in relation to 16. The residual bone height in region was 4 mm in 16 tooth region. Patient was taken-up for direct sinus elevation via lateral window approach for sinus augmentation in relation to 16. Under aseptic conditions and local anesthesia, lateral wall of maxilla was exposed after muco-periosteal flap elevation. A window was created of 1cm diameter corresponding to apical aspect of 16. Sinus membrane was identified and elevated using sinus elevators and reamers without perforating the lining. Once the sinus membrane was elevated, graft material was dispensed to achieve an augmentation of 1cm assessed clinically and confirmed using post-operative OPG. At the end of 6 months, a CBCT scan showed an increased bone height of 12.7 mm. (Figure 6)
Figure 6.Pre-operative and post-operative Orthopantomographs and cross sections of CBCT showing residual alveolar bone height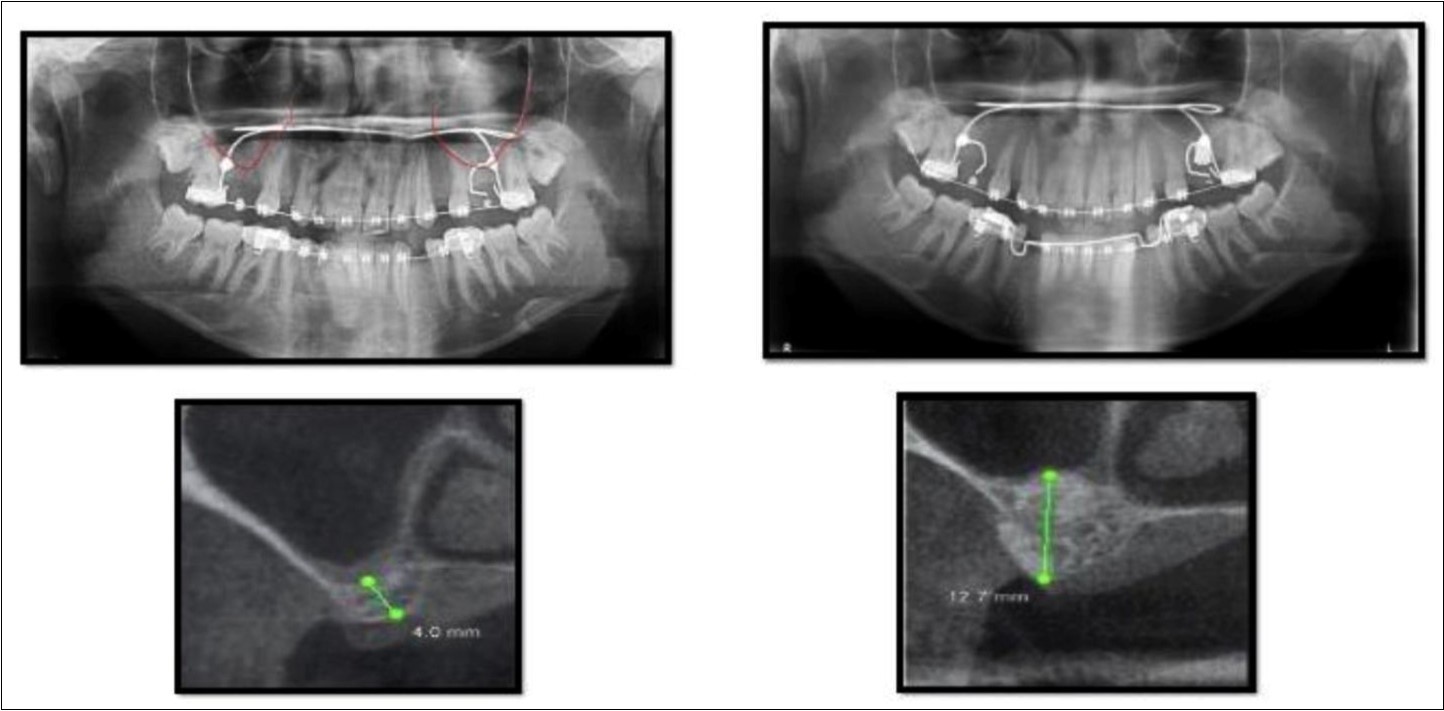
Results
The present study involved evaluation of bone regeneration in terms of increase in residual bone height and bone density following sinus augmentation procedures. It included a total of 20 segments in 17 patients requiring sinus augmentation either by an indirect or a direct approach which was decided based on the residual alveolar bone height on CBCT scans. The study included 9 males and 8 females. The gender distribution in the indirect sinus augmentation procedures was 4 males and 6 females while direct sinus augmentation was done in 6 males and 3 females. 2 patients (one male and one female) underwent both direct and indirect sinus augmentation on their right and left maxillary quadrants and one female underwent direct technique on both sides. The region of sinus augmentation varied from premolar to molar region with the majority of it being in the 1st molar region. In indirect sinus augmentation procedure, as measured by CBCT, the average pre-operative height of bone was 6.8 mm while post-operative height of bone was 11.86 mm. A paired sample t-test was carried-out to know the difference in pre-and post-treatment measurements of bone height with indirect sinus augmentation procedure. The post-treatment bone height (11.86+1.11) was significantly higher than pre-treatment bone height (6.8 +0.70) (t=12.9, p<0.005) (Table 1)
Table 1. Comparison of Mean Pre- and Post-operative Bone Height (in mm) with Indirect Sinus Augmentation as measured by CBCT| Indirect Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| Pre-Operative | 6.8 | 0.7 | 5.06 + 1.24 | 12.9 | <0.005 (Significant) |
| Post-Operative | 11.86 | 1.11 | |||
In direct sinus augmentation procedure, the average pre-operative height of bone was 2.44 mm while post-operative height of bone was 11.27 mm. When a paired sample t-test was carried-out to know the difference in pre-and post-treatment measurements of bone height with direct sinus augmentation, it showed that the post-treatment bone height (11.27 +0.71) was significantly higher than pre-treatment bone height (2.44 +0.81) (t=32.17, p<0.005). (Table 2)
Table 2. Comparison of Mean Pre- and Post-operative Bone Height (in mm) with Direct Sinus Augmentation as measured by CBCT| Direct Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| Pre-Operative | 2.44 | 0.81 | 8.83 + 0.9 | 32.17 | <0.005 (Significant) |
| Post-Operative | 11.27 | 0.71 | |||
In indirect sinus augmentation procedure, as measured by OPG, the average pre-operative height of bone was 7.2 mm while post-operative height of bone was 10.2 mm. A paired sample t-test was carried-out to know the difference in pre-and post-treatment measurements of bone height with indirect sinus augmentation procedure. The post-treatment bone height (10.2+0.92) was significantly higher than pre-treatment bone height (7.2 +1.23) (t=10.06, p<0.005) (Table 3)
Table 3. Comparison of Mean Pre- and Post-operative Bone Height (in mm) with Indirect Sinus Augmentation as measured by OPG| Indirect Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| Pre-Operative | 7.2 | 1.23 | 3.0+ 0.94 | 10.06 | <0.005 (Significant) |
| Post-Operative | 10.2 | 0.92 | |||
In direct sinus augmentation procedure, the average pre-operative height of bone, as measured by OPG, was 1.3 mm while post-operative height of bone was 8.85 mm. When a paired sample t-test was carried-out to know the difference in pre-and post-treatment measurements of bone height with direct sinus augmentation, it showed that the post-treatment bone height (8.85 +1.0) was significantly higher than pre-treatment bone height (1.3 +0.92) (t=19.33, p<0.005). (Table 4)
Table 4. Comparison of Mean Pre- and Post-operative Bone Height (in mm) with Direct Sinus Augmentation as measured by OPG| Direct Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| Pre-Operative | 1.3 | 0.92 | 7.55+ 1.23 | 19.33 | <0.005 (Significant) |
| Post-Operative | 8.85 | 1 | |||
When a comparison was done in the assessment of mean pre-operative height of bone in the indirect sinus augmentation procedure as measured by CBCT and OPG, the average pre-operative height of bone was 6.8 + 0.70 in case of CBCT while 7.2 + 1.23 in case of OPG. When a paired sample t-test was carried-out to know the difference in pre-treatment measurements of bone height with indirect sinus augmentation in case of CBCT and OPG, it showed a p-value of 0.173, which was not significant. (Table 5)
Table 5. Comparison of Mean Pre-operative Bone Height (in mm) with Indirect Sinus Augmentation as measured by OPG and CBCT| Pre-operative Bone Height (in mm) in Indirect Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| OPG | 7.2 | 1.23 | 0.4 + 0.86 | 1.48 | 0.173 (Not significant) |
| CBCT | 6.8 | 0.7 | |||
When a comparison was done in the assessment of mean post-operative height of bone in the indirect sinus augmentation procedure as measured by CBCT and OPG, the average post-operative height of bone was 11.86 + 1.11 in case of CBCT while 10.2 + 0.92 in case of OPG. When a paired sample t-test was carried-out to know the difference in post-treatment measurements of bone height with indirect sinus augmentation in case of CBCT and OPG, it showed a p-value of <0.005, which was significant. (Table 6)
Table 6. Comparison of Mean Post-operative Bone Height (in mm) with Indirect Sinus Augmentation as measured by OPG and CBCT| Post-operative Bone Height (in mm) in Indirect Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| OPG | 10.2 | 0.92 | 1.66 +0.84 | 6.21 | <0.005 (Significant) |
| CBCT | 11.86 | 1.11 | |||
When a comparison was done in the assessment of mean pre-operative height of bone in the direct sinus augmentation procedure as measured by CBCT and OPG, the average pre-operative height of bone was 2.44 + 0.81 in case of CBCT while 1.3 + 0.92 in case of OPG. When a paired sample t-test was carried-out to know the difference in pre-treatment measurements of bone height with indirect sinus augmentation in case of CBCT and OPG, it showed a p-value of <0.005, which was significant. (Table 7)
Table 7. Comparison of Mean Pre-operative Bone Height (in mm) with Direct Sinus Augmentation as measured by OPG and CBCT| Pre-operative Bone Height (in mm) in Direct Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | ||
| Mean | Std. Deviation | t-value | p-value | ||
| OPG | 1.3 | 0.92 | 1.14 + 0.35 | 10.39 | <0.005 (Significant) |
| CBCT | 2.44 | 0.81 | |||
When a comparison was done in the assessment of mean post-operative height of bone in the direct sinus augmentation procedure as measured by CBCT and OPG, the average post-operative height of bone was 11.27 + 0.71 in case of CBCT while 8.85 + 1.0 in case of OPG. When a paired sample t-test was carried-out to know the difference in post-treatment measurements of bone height with indirect sinus augmentation in case of CBCT and OPG, it showed a p-value of <0.005, which was significant. (Table 8)
Table 8. Comparison of Mean Post-operative Bone Height (in mm) with Direct Sinus Augmentation as measured by OPG and CBCT| Post-operative Bone Height (in mm) in Direct Sinus Augmentation | Bone Height (in mm) | Difference | Paired t-test | |||||||
| Mean | Std. Deviation | t-value | p-value | |||||||
| OPG | 8.85 | 1 | 2.42 +0.88 | 8.71 | <0.005 (Significant) | |||||
| CBCT | 11.27 | 0.71 | ||||||||
Discussion
Radiology and imaging plays an important part in any minor or major surgical procedure which is planned. The pre-surgical radiographic assessment allows the surgeon to plan implant insertion in the sub-antral maxillary regions. An accurate pre-surgical planning, based on adequately selected radiology and imaging techniques, ensures optimal surgical results. By bringing new and detailed information through cross-sectional imaging and three dimensional assessment of the region in the pre-surgical phase of treatment, the present study revealed that cone beam computed tomography (CBCT) may change treatment planning for the various sinus lift procedures carried-out in cases with atrophic maxillae and in the presence of numerous other anatomic constraints. There have been a dearth of such studies with statistically significant results comparing the role of conventional radiography, most commonly used, orthopantomography or, panoramic imaging (OPG) and various modalities of cross-sectional imaging including CBCT, which proved the need for the study. Cross-sectional imaging is supposed to influence the treatment planning in such cases at probably all levels including the decision to perform such procedures, sinus anatomy, time of implant placement, the technique used for intervention and the volume of graft material to be used. Radiographic evaluation is necessary for information regarding the quantity and quality of the bone available and to localize anatomic structures in the proximity of the region where the procedure is supposed to be carried-out. Pre-surgical implant imaging should provide information about the implant site with regards to the osseous morphology such as knife edge ridges, cortical irregularities and thickness, developmental variations, enlarged marrow spaces, density of the trabecular bone and post-extraction irregularities in addition to the amount of bone available for implant placement alongwith the orientation of the alveolar bone. Lekholm and Zarb developed a grading scheme for the quality of bone in the proposed implant site in terms of relative proportion and densities of the cortical and medullary bones. According to this scheme, the bone of the alveolar process can be divided into 4 classes:
1.Almost the entire jawbone is composed of homogeneous compact bone;
2.A thick layer of compact bone surrounds a core of dense trabecular bone;
3.A thin layer of compact bone surrounds a core of dense trabecular bone of optimal/favorable strength;
4.A thin layer of compact bone surrounds a core of low density trabecular bone.6
Cross-sectional imaging is required to apply this scheme for implant site assessment. Panoramic imaging has previously been used to study the grafted sinus floors and their relationship with dental implants. However, the position of the maxillary sinus floor was difficult to be assessed on two-dimensional imaging. As cone beam computed tomography (CBCT) has numerous advantages over conventional radiography as well as computed tomography (CT), we included CBCT for carrying-out the intended sinus augmentation procedures, this being in accordance with the study conducted by Temmerman et al in 2011 which showed that panoramic imaging underscored the mesio-distal distance of the available bone in upper premolar region and concluded the need for going for cross-sectional imaging like CBCT for pre-surgical treatment planning in carrying-out such procedures.7 In the present study, our measurements (based on CBCT imaging) pre-operatively and post-operatively for indirect sinus augmentation procedures were 6.8mm and 11.76mm respectively while for direct augmentation procedures, the values were 2.44mm and 11.7mm respectively. The mean of difference in bone height in direct and indirect sinus augmentation procedures was 8.83mm and 4.96mm, the difference obtained being statistically significant with p < 0.005. Arias-Irimia et al measured the volume of sinus lifts post-operatively using CBCT imaging and showed a correlation between the volume of the sinus lift required and the size of the bone graft to be used (height, length).8 There are several studies that have evaluated bone formation after sinus lift procedures and demonstrated the aptness of CBCT imaging for the post-operative evaluation of sinus lift. According to Baciut et al, CBCT increases the accuracy of both assessment of sinus morphology as well as harvesting of bone grafts in line with the estimated volume available.9 CBCT provides three dimensional imaging in the maxillofacial region at relatively low radiation doses as compared to the conventional CT. Also, because of these inherent advantages over conventional CT and two dimensional radiography, CBCT was recommended in our study for the evaluation of residual alveolar bone height as an easy and effective way of measuring the pre-and post-operative bone heights.10 A study by Nishida et al involved 52 patients with bone height of less than 8mm in maxillary posterior region. The study utilized CBCT imaging to assess the radiographic appearance of bone graft domes longitudinally after osteotome sinus floor elevation. Implants (𝑛 = 91) were subsequently placed in regenerated bone following osteotome sinus floor elevation while autogenous bone was used as the augmentation graft material. Radiographic findings after a 6 month follow-up revealed that atleast 1mm of grafted augmentation material was recognized around the implant fixtures on CBCT scans at the time patient had reported for the second phase of implant placement. Also, the border between the grafted augmentation material and the existing bone was found to be indistinct while the grafted area apical to implants was seen to undergo shrinkage and remodelling suggesting sufficient grafted autogenous bone changes that were required to be obtained as an outcome of the treatment for a successful implant procedure to be carried-out.11 Soardi et al in 2014 did a quantitative comparison of CBCT and micro-radiography in the evaluation of bone density after maxillary sinus augmentation procedures by conducting a two-stage protocol in 19 consenting patients, all having the crestal bone less than 2mm. A succession of CBCT images of the maxilla were taken before surgery, after the sinus augmentation procedure, and immediately after implant insertion. Also, bone core biopsy was taken at the site of implant placement 6 months after the surgical procedure. The authors concluded that CBCT imaging had a clear predictability in the treatment planning.12 A single case on sinus augmentation was reported by Kumar et al in 2013 who opted for CBCT imaging for the pre-operative evaluation of the left maxillary posterior region. The CBCT scans of this 52 year old woman revealed a bone height ranging from 4.1mm-5.4mm in the left maxillary posterior region. This patient underwent direct sinus lift procedure. The results were highly satisfactory showing regeneration upto approximately 13mm.13 Regardless of the material or surgical technique used for sinus grafting, a pre-operative clinical and radiological examination including the conventional panoramic radiography and/or, CT or CBCT, should always be done for the planning of surgery and implant placement.14 Panoramic radiography displays an inherent deformation which impedes its interpretation and exact quantitative measurements. Rodriguez-Recio et al have shown the benefits of using CT and specialized software that can provide important information about the quality and quantity of bone in the palatal donor areas.15 Baena et al performed a radiographic evaluation of regenerated bone following poly (lactic-co-glycolic) acid/hydroxyapatite and de-proteinized bovine bone graft in various sinus lift procedures. The vertical height of the bone and density were assessed at approximately 28 weeks after grafting using panoramic imaging (only for vertical height of bone) and cone beam computed tomography. The vertical dimension of the regenerated bone was equivalent between the 2 groups. In our study, we conducted paired sample t-test to know the difference in original and grafted sinus floor measurements for bone density (Gray scale values) in case of both direct as well as indirect sinus augmentation procedures and found extremely promising results which were found to be statistically significant (p<0.001). The outcome of this study suggests that CBCT can be used for analysis of bone quantity and quality and in predicting the success of grafts in direct and indirect sinus augmentation procedures. When analyzing all types of images, the examiners chose to indicate different procedures. When planning in three dimension, a surgeon can examine details in sinus morphology for accurate graft-and implant-placement sites. By changing the treatment alternative, after the initial observations and surgical plans had been made, the predicted complications could as such already be dealt with. The surgical procedure selection was performed according to the residual alveolar bone/crestal bone height (in view of the rigid fixation when using simultaneous implantation) and minimal invasiveness. In any sinus lift procedure for a successful implant placement, there is always a need felt to reduce surgical risks, invasiveness, cost and time while simultaneously performing the best suited surgical procedure to exploit most of the existing bone and morphology for the purpose of implant placement. In this, a key point in cross-sectional imaging is in the aptness achieved in the evaluation of a deficient crest and comparison of the original and post-augmentation dimensions.3An accurate estimation of the necessary bone graft volume is very important in order to optimize the surgical technique and to reduce risk of impending complications. Buyukkurt et al showed that three dimensional CT techniques can be used to calculate the volume required for sinus floor augmentation procedures.16 This study evaluated the clinical validity of CBCT in comparison to panoramic radiography regarding pre-operative implant planning in combination with sinus grafting procedures and assessed the accuracy of CBCT for pre-operative estimation of the required sinus lift height and in the estimation of the volume of grafting material required for sinus grafting procedures. The results proved that using specialized software, CBCT allows the estimation of the height for bone grafts significantly better than panoramic radiography. Therefore, within the limitations of the present study, CBCT seems to be a superior examination technique because of the provision for three dimensional planning. Several studies have shown the benefits of using CT that can provide important volumetric information about the quality and quantity of bone in the palatal donor area.15,17 Complications are determined by a complex interaction of intra-operative factors and cannot be fully predicted by any radiological examination. Nevertheless, in our case also, few patients were encountered wherein the treatment choice was adapted after having CBCT imaging. In a clinical context, this treatment switch might have prevented complications or unexpected events during surgery. Indeed, instead of a bone shortage revealed during surgery, requiring a sudden change in treatment strategy, this bone shortage could be detected prior to surgery, giving the intervention an optimal set-off. There are several studies that evaluate bone formation after sinus lift procedures demonstrating the usefulness of CBCT for post-operative evaluation of sinus lift procedures also.18,19
Conclusion:
Based on the findings of the above study, it can be concluded that CBCT has an important role in cases of sinus lift procedures to improve the diagnostic efficiency as well as the accuracy of sinus lift procedures. In addition, it is extremely helpful in the pre-surgical planning of the sinus lift procedures and for an efficient comparison of the gain in vertical alveolar bone height post-graft placements. When only panoramic radiographs are used, bone quantity and quality are risked to be over-estimated. The present study demonstrates that CBCT increases the accuracy of both, the sinus morphology assessment as well as the estimation of gain in vertical alveolar bone height, in addition to bone density, which remains unassessed by conventional radiological techniques.
References
- 1.White S C, Pharoah M J. (2013) Oral Radiology: Principles and Interpretation: Elsevier-Health Sciences Division.
- 2.Chan H L, Misch K, Wang H L. (2010) Dental imaging in implant treatment planning. Implant Dentistry;19: 288-298.
- 3.Temmerman A, Hertelé S, Teughels W, Dekeyser C, Jacobs R et al. (2011) Are panoramic images reliable in planning sinus augmentation procedures. Clinical Oral Implants Research2011;. 22, 189-194.
- 4.Misch C E. (2008) Contemporary Implant Dentistry: Mosby Elsevier;2008.72.Moore WR, Graves SE, Bain GI. Synthetic bone graft substitutes. , ANZ Journal of Surgery2001;71: 354-361.
- 5.Tatum H Jr. (1986) Maxillary and sinus implant reconstructions. , Dental Clinics of North America1986; 30, 207-229.
- 6.Keeting P E, Scott R E, Colvard D S, Anderson M A, Oursler M J et al. (1992) Development and characterization of a rapidly proliferating, well-differentiated cell line derived from normal adult human osteoblast-like cells transfected with SV40 large T antigen. , Journal of Bone and Mineral Research: The Official Journal of the American Society for Bone and Mineral Research1992; 7, 127-136.
- 7.Arias-Irimia O, Barona-Dorado C, Martínez-Rodríguez N, Ortega-Aranegui R, Martínez-González J. (2010) Pre-operative evaluation of the volume of bone graft in sinus lifts by means of CompuDent. Medicina Oral Patologia Oral y Cirurgia Bucal. 15, 512-516.
- 8.Baciut M, Hedesiu M, Bran S, Jacobs R, Nackaerts O et al. (2013) Pre- and post-operative assessment of sinus grafting procedures using cone-beam computed tomography compared with panoramic radiographs. Clinical Oral Implants Research2013;. 24, 512-516.
- 9.Pjetursson B E, Tan W C, Zwahlen M, Lang N P. (2003) A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. , Journal of Clinical Periodontology2008; 35, 216-240.
- 10.Block M S, Kent J N. (1997) Sinus augmentation for dental implants: The use of autogenous bone. , Journal of Oral and Maxillofacial Surgery, The Official Journal of the American Association of Oral and Maxillofacial Surgeons1997; 55, 1281-1286.
- 11.Resnik L, Liu D, Hart D L, Mor V.Benchmarking physical therapy clinic performance: Statistical methods to enhance internal validity when using observational data. Physical therapy 2008;88:. 1078-1087.
- 12.Smiler D G, Johnson P W, Lozada J L, Misch C, Rosenlicht J L et al. (1992) Sinus lift grafts and endosseous implants: Treatment of the atrophic posterior maxilla. , Dental Clinics of North America1992; 36, 151-186.
- 13.Reddy M S, Mayfield-Donahoo T, Vanderven F J, Jeffcoat M K. (1994) A comparison of the diagnostic advantages of panoramic radiography and computed tomography scanning for placement of root form dental implants. Clinical Oral Implants Research1994;. 5, 229-238.
- 14.Rodriguez-Recio O, Rodriguez-Recio C, Gallego L, Junquera L. (2010) Computed tomography and computer-aided design for locating available palatal bone for grafting: Two case reports. The International Journal of Oral and Maxillofacial Implants2010; 25, 197-200.
- 15.Buyukkurt M C, Tozoglu S, Yavuz M S, Aras M H. (2010) Simulation of sinus floor augmentation with symphysis bone graft using three dimensional computerized tomography. , The International Journal of Oral and Maxillofacial Surgery2010; 39, 788-792.
- 16.Liang X, Jacobs R, Hassan B, Li L, Pauwels R et al. (2010) A comparative evaluation of cone beam computed tomography (CBCT) and multi-slice CT (MSCT): Part I. On subjective image quality. , Eur Radiol2010; 75, 265-269.
- 17.Liang X, Lambrichts I, Sun Y, Denis K, Hassan B et al. (2010) A comparative evaluation of cone beam computed tomography (CBCT) and multi-slice CT (MSCT). Part II: On 3D model accuracy. Eur Radiol. 75, 270-274.
Cited by (3)
This article has been cited by 3 scholarly works according to:
Citing Articles:
Research Square (Research Square) (2025) OpenAlex
BioMed Research International (2021) OpenAlex
BioMed Research International (2021) Crossref