
Evaluation of an External Quality Assessment Program for HIV Testing in Tigray North Ethiopia 2016
Abstract
Background:
Point-of-care diagnostic tests (POCTs) are increasingly used in both developing and developed countries. They allow same day testing and treatment at remote locations where no laboratory support is available. Quality control measures, which are routinely used in laboratories, have not been widely implemented for POCTs. This aimed to assess the integrity of the entire laboratory testing process, and aims to educate and improve performance in quality of HIV rapid testing.
Methods:
A health facility based cross section study was conducted from April to June 2016.Randomly selected health facilities were participated in the external quality assessment. Onsite evaluation and panel test were used to collect data using structured checklists and formats. Data was entered and analyzed using SPSS version 16.
Results:
Between April to June 2016, a total of 60 health facilities (145 testing points) from governmental health facilities (hospitals and health centers) were participated in the study. Among the participated testing points 41% have no designated area, 40% have no clean water for hand washing and 51% have no national test algorithm. The average performance of testing points was varies from 89.6% to 99.1% (Laboratory 99.1%, ANC 90.4%, TB clinic 91.4% and VCT 89.6%). In a multivariable logistic regression model, didn’t follow national testing algorithm to report client test results have statistical significance.
Conclusions:
High quality test results underpin accurate diagnosis and appropriate treatment for patients. But in the study area the score of proficiency testing result and coverage of training is slightly low comparing to other findings. Therefore following national testing algorithm to report client test results, training and monitoring are critical points to improve the proficiency testing score of testing points.
Author Contributions
Academic Editor: Tsegahun Manyazewal, Center for Innovative Drug Development and Therapeutic Trials for Africa (CDT - Africa)
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Gebrehiwet Tesfahuneygn, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Background
Point-of-care diagnostic tests (POCTs) are increasingly used in both developing and developed countries 1. They allow same day testing and treatment at remote locations where no laboratory support is available. Quality control measures, which are routinely used in laboratories, have not been widely implemented for POCTs. The World Health Organization and US Centers for Disease Control and Prevention advocates the implementation of POCT with a quality assurance method in place 2.
The World Health Organization (WHO) defines External Quality Assessment (EQA) as a system for objectively checking a laboratory’s performance using an external agency or facility 3. EQA participation is associated with improved laboratory performance over time and is a requirement for accreditation 4. However, many professionals in Sub-Saharan Africa (SSA) countries are unable to effectively implement quality improvement programs and many countries remain without an accredited clinical laboratory 5. Establishing, maintaining and demonstrating the accuracy of diagnostic tests is a major challenge for most laboratories in SSA, and the complexity and cost of setting up and main training quality assurance systems mean that very few laboratories, mainly tertiary or privately owned, can achieve these standards 6, 7. The common perception that EQA is costly or unnecessary has hindered the widespread enrolment of laboratories into EQA programs 8.EQA can be applied in three main ways, each with advantages and disadvantages: 1) Proficiency testing (PT), where an external provider sends samples of undisclosed results to laboratories or individual testers and provides feedback on results; 2) Rechecking or retesting samples in higher level or peer laboratories (inter-laboratory comparison); 3) On-site assessment by approved evaluators 3.
Health service utilization to human immunodeficiency (HIV) has expanded rapidly in Ethiopia. National efforts to scale up care and treatment services for individuals with HIV depend on efficient laboratory services, including HIV testing, which is the main entry point to access to care and treatment. In spite of increased access to HIV counseling and testing in developed countries, most people living with HIV in low and middle-income countries are unaware of their aerostats 9.
While available rapid diagnostic tests (RDTs) for HIV have high sensitivity and specificity when performed correctly, incorrect use can result in incorrect results, with serious consequences 10. EQA is critical to assess the quality of laboratory performance and to ensure accuracy and reliability of laboratory results 11.This aimed to assess the integrity of the entire laboratory testing process, to educate and improve performance in quality of HIV rapid testing.
Methods
Study Area
The study was conducted in Tigray region which is located at a distance of 600 km northeast of Addis Ababa. Tigray is bordered by Eritre to the north, Suda to the west, the Afar Regio to the east, and the Amhara Regio to the south and southwest.
Study Design, Period and Study Subject
A health facility based cross section study was conducted from April to June 2016.Randomly selected health facilities were selected. Sixty hospitals and health centers (145 testing points) were participated in this study.
Data Collection and Quality Control Methods
Proficiency test, standard checklist and on site observation were used during the specified time to asses overall quality HIV rapid test including HIV testing, HIV testing methods used, utilization of standard operating procedures (SOPs), internal and external quality control utilization.
Data Processing and Analysis
The quality of data was checked by reviewing the questionnaire for consistency and completeness. Data were entered, cleared and analyzed using SPSS version 16.
Result
A total of 145 testing points from governmental health facilities (hospitals and health centers) participated in the study. Among the participated testing points 41% have no designated area, 40% have no clean water for hand washing and 51% have no national test algorithm (Table 1).
Table 1. General back ground characteristics of testing points in HIV testing| characteristics | Yes N (%) | No N (%) |
| Designated area for HIV testing | 86 (59) | 59 (41) |
| Availability of clean water and soap for hand washing | 87 (60) | 58 (40) |
| Availability of national test algorithm | 94 (64.8) | 51 (35.2) |
| Sop for each HIV rapid test | 72 (49.7) | 73 (50.3) |
| Kits and supplies used within their expiry date | 139 (96) | 6 (4) |
| IQC practice | 65 (45) | 80 (55) |
| Training for HIV rapid test | 81 (56) | 64 (44) |
| Clean and organized working area | 132 (91) | 13 (9) |
| Appropriate disinfectants | 110 (76) | 35 (24) |
| Waste segregation | 101 (70) | 44(30) |
| kits stored according to manufacturer recommendation | 137 (94.5) | 8 (5.5) |
| Inventory management | 59 (41) | 86 (59) |
| job aids on specimen collection | 52 (36) | 93 (64) |
| Availability of sufficient kits and supplies | 122 (84) | 23 (16) |
| Labeling with client identification number | 12 (89) | 16 (11) |
| Availability of timer | 44 (30) | 101 (70) |
| testing procedures adequately followed | 108 (74.5) | 37 (25.5) |
| Following the national testing algorithm to report the client test result | 128 (88) | 17 (12) |
PT Result of Testing Points
Most (82.8%) of the testing points score above the expected standard. From the total testing points 118 (81.4%) testing points score 100%, 6 (4.2%) testing points score 33%, 19 (13%) testing points score 67% and 2 (1.4%) testing points score 83%. The average performance of testing points was varies from 89.6% to 99.1(Laboratory 99.1%, ANC 90.4%, TB 91.4% and VCT 89.6%).
Factors Associated with Poor HIV Rapid test PT Performance
In a univariable logistic regression analysis, have no national algorithm in testing sites has high risk (odd ratio 2.86) to report false client results than having national test algorithm at P value (0.03). Using timer to report client result has reduced false HIV results six times than not using timer (P value 0.015). An adequately following test procedure during HIV testing has great advantage. Because it reduces false negative results 4 times than not adequately following test procedure (P value 0.002) (Table 2).
Table 2. Association of health service providers with HIV rapid test PT results| Characteristics | Response categories | PT result | Crude OR (95% CL) | P-value | |
| Meet the standard | Below the standard | ||||
| Testing points | laboratory | 36(97.3) | 1(2.7) | Reference | |
| ANC | 29(76.3) | 9(23.7) | 11.172(1.34, 93.37) | .026 | |
| TB | 29(82.9) | 6(17.1) | 7.45(.85, 65.41) | .070 | |
| VCT | 26(74.3) | 9(25.7) | 12.462(1.486, 104.51) | .020 | |
| Availability of national test algorithm | Yes | 83(88.3) | 11(11.7) | Reference | |
| No | 37(72.5) | 14(27.5) | 2.86(1.19,6.89) | .019 | |
| Sop for each HIV rapid test | Yes | 64(88.9) | 8(11.1) | Reference | |
| No | 56(76.7) | 17(23.3) | 2.43(.97,6.10) | .057 | |
| Kits and supplies used within their expiry date | Yes | 115(82.7) | 24(17.3) | Reference | |
| No | 5(83.3) | 1(16.7) | .96(.11,8.60) | .97 | |
| IQC practice | Yes | 59(90.8) | 6(9.2) | Reference | |
| No | 61(76.2) | 19(23.8) | 3.06(1.14,8.20) | .026 | |
| Training for HIV rapid test | Yes | 67(82.7) | 14(17.3) | Reference | |
| No | 53(82.6) | 11(17.2) | .99(.42,2.37) | .99 | |
| kits stored according to manufacturer recommendation | Yes | 115(83.9) | 22(16.1) | ||
| No | 5(62.5) | 3(37.5) | 3.14(.70,14.10) | .14 | |
| job aids on specimen collection | Yes | 48(92.3) | 4(7.7) | Reference | |
| No | 72(77.4) | 21(22.6) | 3.50(1.13,10.83) | .030 | |
| Labeling with client identification number | Yes | 110(85.3) | 19(14.7) | Reference | |
| No | 10(62.5) | 6(37.5) | 3.47(1.13,10.68) | .030 | |
| Availability of timer | Yes | 42(95.5) | 2(4.5) | Reference | |
| No | 78(77.2) | 23(22.8) | 6.17(1.39,27.55) | .017 | |
| testing procedures adequately followed | Yes | 96 | 12 | Reference | |
| No | 24 | 13 | 4.3(1.8,10.7) | .002 | |
| Following the national testing algorithm to report the client test result | Yes | 111(86.7) | 17(13.3) | Reference | |
| No | 9(52.9) | 8(47.1) | 5.80(1.97,17.10) | .001 | |
| characteristics | Response categories | PT result | Crude OR (95% CL) | Adjusted OR (95% CL) | P-value | |
| Meet the standard | Below the standard | |||||
| Testing points | laboratory | 36(97.3) | 1(2.7) | Reference | Reference | |
| ANC | 29(76.3) | 9(23.7) | 11.172(1.34, 93.37) | 3.58(.30,42.22) | .311 | |
| TB | 29(82.9) | 6(17.1) | 7.45(.85, 65.41) | 2.70(.20,35.05) | .454 | |
| VCT | 26(74.3) | 9(25.7) | 12.46 (1.49, 104.51) | 5.71(.46,71.01) | .175 | |
| Availability of national test algorithm | Yes | 83(88.3) | 11(11.7) | Reference | Reference | |
| No | 37(72.5) | 14(27.5) | 2.86(1.19,6.89) | 2.06(.69,6.22) | .198 | |
| IQC practice | Yes | 59(90.8) | 6(9.2) | Reference | Reference | |
| No | 61(76.2) | 19(23.8) | 3.06(1.14,8.20) | 1.80(.50,6.52) | .374 | |
| job aids on specimen collection | Yes | 48(92.3) | 4(7.7) | Reference | Reference | |
| No | 72(77.4) | 21(22.6) | 3.50(1.13,10.83) | 1.70(.38,7.68) | .492 | |
| Labeling with client identification number | Yes | 110(85.3) | 19(14.7) | Reference | Reference | |
| No | 10(62.5) | 6(37.5) | 3.47(1.13,10.68) | 2.05(.48,8.74) | .332 | |
| Availability of timer | Yes | 42(95.5) | 2(4.5) | Reference | Reference | |
| No | 78(77.2) | 23(22.8) | 6.17(1.39,27.55) | 3.17(.45,22.18) | .246 | |
| testing procedures adequately followed | Yes | 96 | 12 | Reference | Reference | |
| No | 24 | 13 | 4.3(1.8,10.7) | 1.29 (.35,4.73) | .701 | |
| Following the national testing algorithm to report the client test result | Yes | 111(86.7) | 17(13.3) | Reference | Reference | |
| No | 9(52.9) | 8(47.1) | 5.80(1.97,17.10) | 11.57(2.46,54.35) | .002 | |
In a multivariable logistic regression model, didn’t follow national testing algorithm to report client test results has statistical significance (Table 3).
Discussion
External quality assessments is a method used for assessing laboratory and health care professionals’ performance and allows for the evaluation of inter-laboratory proficiency tests and the identification of related problems. Accordingly, it affords grounds for corrective and preventive actions on a regular basis 10. Measures to control the quality of result in HIV diagnostic laboratories are extremely important, because of the consequence of either false Positive or false negative results are huge 9.
This study demonstrates low (56%) coverage of HIV training in the testing points. This is different from a study conducted in south Ethiopia which was 85% 11. This difference may be due to difference in sample size and characteristics of study participants, our study participants were laboratories and other health professionals whom perform HIV rapid test in TB clinic, VCT, ANC but their study participants were only laboratory and their samples were only 20 health facilities. From the assessed testing points, 64 (44%) health professionals’ who conduct HIV testing were found to have no trained in HIV testing. This is incomparable with study conducted in Ethiopia, which reported only14% were found to have no trained in HIV testing 11. In this study 12% study participants didn’t follow national test algorithm. This is in line with study conducted in Ethiopia, which demonstrates 10% of the study participants didn’t follow national test algorithm. Our finding demonstrated that 50% testing points have no SOP for each testing points. In contrast to this findings study conducted in Ethiopia and South East Asia reported that from assessed laboratories 0% and 8% did not have SOPs respectively 11, 12.
The average score of the testing points were 92.7%. Figure 1 This slightly lower than nine year survey conducted in Africa WHO region which indicated that 98.9% 13. This deference may be due to study participant difference and method used for HIV testing. Because our study participants included all testing points and they performed HIV testing using HIV rapid test but their study participants’ only laboratory professionals and they used HIV rapid test and ELISA to perform HIV rapid testing. Our findings demonstrated that 82.8% of testing points score 80 and above this lower than study conducted by Jean Louis and his colleagues which was 97.5% 14.
Figure 1.Average performance of testing points in %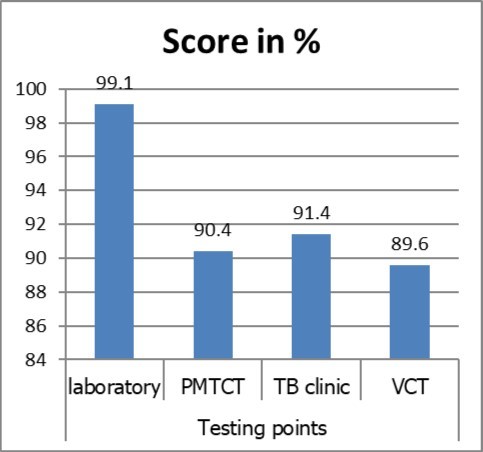
Conclusions and Recommendations
High quality test results underpin accurate diagnosis and appropriate treatment for patients. But in the study area the score of PT result and coverage of training is slightly low comparing to other findings. Therefore following national testing algorithm to report client test results, training and monitoring are critical points to improve the PT score of testing points.
Declaration
Ethical Approval and Consent to Participate
Ethical approval was obtained from Tigray regional health bureau and permission was obtained from each health facilities before conducting this study.
Consent to Publish
Not applicable
Availability of Data and Materials
All data and materials are available in SPSS and excel. We can avail our raw data for all who need it.
Funding
Not applicable
Authors’ Contribution
GT and GG designed the study, participated in data collection, analysis, interpretation, and write-up, drafted the manuscript and critically revised the manuscript. Both authors read and approved the final manuscript.
Acknowledgements
We would like to acknowledge Tigray health bureau, Tigray health research institute and we also like to thanks to each health facility heads and laboratory staffs.
References
- 1.Gillet P, Mukadi P, Vernelen K, M Van Esbroeck, Muyembe J J et al. (2010) External quality assessment on the use of malaria rapid diagnostic tests in a non-endemic setting. , Malar J 9, 359-2.
- 2. (2005) Guidelines for Assuring the Accuracy and Reliability of HIV Rapid Testing: Applying a Quality System Approach. Atlanta, GA: Centers for disease control and prevention;.
- 3.World Health Organization. (2011) Overview of external quality assessment (EQA): module 10, content sheet 10-1.WHO,Geneva,Switzerland. Available at:http://www.who.int/ihr/training/laboratory_quality/10_ b_eqa _contents.pdf.AccessedApril3rd2016.
- 4.Noble M A. (2007) Does external evaluation of laboratories improve patient safety? Clin Chem Lab Med.https://doi.org/10.1515/CCLM.2007.166. 45, 753-5.
- 5.Mesfin E A, Taye B, Belay G, Ashenafi A. (2015) The status of medical laboratory towards of AFRO WHO accreditation process in government and private health facilities in Addis Ababa. , Ethiopia. https://doi.org/10.11604/pamj.2015.22.136.7187, Pan African Med J 22, 136.
- 6.Bates I, Maitland K. (2006) Are laboratory services coming of age in sub-Saharan Africa? Clin Infect Dis.https://doi.org/10.1086/499368. 42, 383-4.
- 7.Kibet E, Moloo Z, Ojwang P J, Sayed S, Mbuthia A et al. (2014) Measurement of improvement achieved by participation in international laboratory accreditation in sub-Saharan Africa. The Aga Khan University Hospital Nairobi experience. https://doi.org/10.1309/AJCPV8A9MRWHGXEF. , Am J ClinPathol 141, 188-95.
- 8.Peter T, Badrichani A, Wu E, Freeman R, Ncube B et al. (2008) . Challenges in implementing CD4 testing in resource-limited settings.CytometryB ClinCytom.https://doi.org/10.1002/cyto.b.20416. 74B: S123–130
- 9.Alemnesh H, Mirkuzie G, Hinderaker O.Promising outcomes of a national program for the prevention of mother-to-child HIV transmission in Addis Ababa: a retrospective study BMC Health services Research. 1472-6963.
- 10.Yao K, Wafula W, Bile E C. (2010) Ensuring the quality of HIV rapid testing in resource-poor countries using a systematic approach to training. , Am J ClinPathol 134, 568-572.
- 11. (2013) World Health Organization (WHO)/UNAIDS. Guidelines for Organizing National External Quality Assessment Schemes for HIV Serological Testing. www.who.int/diagnostics_laboratory/quality/en/EQAS96.pdf
- 12.Regasa Belayneh. (2014) Assessment of Quality Assurance Program of HIV Testing in Ethiopia. , AmJ of InteMedi 2(6), 106-108.
Cited by (4)
This article has been cited by 4 scholarly works according to:
Citing Articles:
BMC Infectious Diseases (2023) Crossref
Dereje Yenealem, Shemsu Kedir, Asmare MekonnenWubie, Daniel Melese, Tamirat Molalign et al. - BMC Infectious Diseases (2023) Semantic Scholar
BMC Infectious Diseases (2023) OpenAlex
Research Square (Research Square) (2022) OpenAlex
Journal of Clinical Research in HIV AIDS and Prevention (2017) OpenAlex