
Human Immunodeficiency Virus Drug Resistance (HIVDR) and Baseline Characteristics among Antiretroviral Therapy (ART) experienced Children and Adolescents under the care of Chidamoyo Christian Hospital in Hurungwe, Zimbabwe
Abstract
Introduction
Human Immunodeficiency Virus (HIV) remains a persistent global public health challenge. In 2020, approximately 37.9 million individuals were living with HIV globally, including 1.7 million children <15 years old, with a global HIV prevalence of 0.8% among adults. A larger portion of people living with HIV are found in low-and middle-income countries, and Sub-Saharan Africa (SSA) is home to about 68% of people living with HIV in the world. Strikingly, with increased uptakes in PMTCT, challenges in ART programs, and high viremia among children and adolescents in SSA, the success rate of ART might be quickly compromised, with possible HIVDR emergence, particularly after years of paediatric ART exposure. Therefore, monitoring ART response in children and adolescents in terms of HIVDR patterns and other socio-economic determinants of disease progression might help achieve better treatment outcomes at individual levels. At a programmatic level, this can guide further optimization of treatment options for SSA especially Zimbabwean rural where there is paucity of information on HIVDR prevalence in children and adolescents.
Methods
We enrolled 89 children and adolescents experiencing virologic failure from Chidamoyo Christian Hospital in Hurungwe. We managed to amplify all the 89 using nested PCR and 32.5% (29) had resistance to at least one ART drug and analysis was done using the 29 samples.
Results
Among the 89 participants with virologic failure,29 were resistant to at least one of their ART drugs. 39.2% of males and 23.07% of females had HIV-1 with resistance to at least one medication. Among 29 participants with HIVDR mutations, the prevalence of at least one HIVDR mutation to protease inhibitors (PIs), Nucleotide Reverse Transcriptase Inhibitors (NRTI), and Non-Nucleotide Reverse Transcriptase Inhibitors (NNRTI) were 6.47% ,46.76% and 46.76% respectively. Of the 29 participants who had HIVDR 19 (65.5%) had resistance to a drug they were currently taking and they needed to be switched to a better effective ART regimen
Conclusion
Use of HIVDR testing in guiding and monitoring development of HIVDR at the start of ART or at 1st failure can be very important in treatment options and patient management.
Article Information
- Received
- Accepted
- Published
Copyright © 2023 Alfred Makura, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Alfred Makura, Biomedical Research and Training Institute, University of Zimbabwe, College of Health Sciences, Department of Chemical Pathology, Vitralabs, Clinical Diagnostic Centre, 55 King George, Avondale, Harare, Zimbabwe —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Background
Human Immunodeficiency Virus (HIV) remains a persistent global public health challenge. In 2020, approximately 37.7 million (30.2–45.1 million) individuals were living with HIV globally, including 1.7 million children <15 years old, with a global HIV prevalence of 0.8% among adults1. Almost 74.9 million individuals have been infected with HIV and 32.0 million have died from AIDS-related illnesses from the time when the epidemic started. A larger portion of people living with HIV(PLWH) are found in low- and middle-income countries, and Sub-Saharan Africa (SSA) is home to about 68% of people living with HIV in the world 2. Among this group, 20.6 million reside in East and Southern Africa which recorded 800,000 new HIV infections in 2018 (ref). The use of combination antiretroviral therapy (cART) in the treatment and management of HIV patients has lowered the risk of HIV-1 transmission, morbidity and mortality. Data from 2019 indicated that 25.33 million PLWH were receiving cART worldwide. However, mortality rates are still high in populations residing in resource-limited settings especially in the first months on cART as a result of late diagnosis and an already depleted. A meta-analysis of 63 studies conducted in low and middle income countries (LMICs) indicated that HIV drug resistance in persons before the start of cART (pre-treatment HIVDR or PDR) has steadily increased worldwide from 2000 to 2016, coincident with the wide-scale roll out of ART4.A systematic literature review on HIVDR resistance in 8 LMICs found that, in 60% of patients experiencing ART failure after 12 months of initiation, there were resistance mutations to at least 1 ART drug class5. Other studies reported that, in HIV-1–infected infants aged between 2.5 months - 8 years in SSA who were exposed to ART for prevention of mother-to-child transmission (PMCT), close to 32.4% had virus resistant to non- nucleoside reverse transcriptase inhibitors (NNRTIs)6. Around 86% of adolescents and young adults experiencing virologic failure had HIVDR in Zimbabwe 5, 6, 7, 8.HIVDR contributes to increased costs of HIV-1 care. Unfortunately, in Zimbabwe, HIVDR testing is not routinely done especially in children and adolescents and it might be one of the major causes of treatment failure among this special group.
Strikingly, with increased uptakes in PMTCT, challenges in cART programs, and high viremia among children and adolescents in SSA, the success rate of ART might be quickly compromised, with possible HIVDR emergence, particularly after years of paediatric cART exposure. Therefore, monitoring ART response in children and adolescents in terms of HIVDR patterns and socio-economic determinants of treatment failure might limit disease progression and guide on subsequent cART options for SSA especially Zimbabwean rural where there is paucity of information on HIVDR prevalence in children and adolescents.
We thus analysed baseline enrolment data collected through a randomized controlled study entitled Community Based ART (CBART) in order to determine the baseline characteristics and then genotyped plasma samples to determine the prevalence and distribution of HIVDR resistance among ART- experienced children and adolescents, aged 10 to 19 years, attending Chidamoyo Christian Hospital in Hurungwe, Zimbabwe
Methods
The study was nested in the CBART randomized control clinical trial .This was cohort study under Biomedical Research and Training Institute (BRTI), whose main objective as to determine if Implementation of point of care virus load differentiated care (POC virus load), targeted genotyping and Ministry of Health tools will result in improved virologic suppression among children, adolescents and young adults (<25 years) on ART.”The CBART study enrolled 600 cART experienced children and adolescents (10 to 19 years) over a period of two years (2018 to 2020).
In the original study, all eligible ART patients under the care of Chidamoyo Christian Hospital (< 25 years of age) were requested to consent to participate in the study at their regular cART visits. At the beginning of the study, the Ministry of Health and Child Care Zimbabwe (MOHCZ) was rolling out a new standard of care (SOC) which included annual virus load monitoring using the Roche Cobas HIV-1 RNA quantification (Roche Diagnostics, CA, USA) through the Provincial Laboratory at Chinhoyi (100 km from Chidamoyo). Four-hundred and fifty HIV infected children and adolescents and young adults (CAY) on cART were randomized (1:1) at enrolment to either SOC (n=300) or a near POC (n=300) VLDC monitoring test. All those who consented to CBART were offered the SOC VL performed by Roche COBAS at Chidamoyo and the results were returned to the hospital within 2-4 weeks of testing. Follow-up testing for HIV RNA > 1,000 copies/ml was offered using the same virologic monitoring system at the next drug/clinic visit within 3 months.
Participants recruitment, data collection and follow up were carried from January 2018–March 2020 in Hurungwe District, Mashonaland West Province, Zimbabwe. Hurungwe is comprised of mainly rural areas, with an economy centred on agriculture (mainly tobacco and cotton farming). Mashonaland West Provinces has the fourth highest HIV prevalence in Zimbabwe. A total of 3 223 new HIV infections were recorded in 2016 in Mashonaland West, out of which 4% were children below the age of 14. The study was conducted at Chidamoyo Christian Hospital in Hurungwe which serves about 30000 people and is an important referral centre for neighbouring areas such as Siakobvu, Kariba and Karoi. The hospital has over 18 outreach Opportunistic Infection (OI) clinics where they deliver ART drugs. However, 8 sites were used for this sub-study. The choice of the Institution for the study was based on its high HIV burden, its high coverage of cART, the long-term experience in ART provision of health facilities, hence need to assess HIVDR. In this sub-study,89 participants with viral load above 1000 copies per millilitre (VL>1000 copies/Ml) where enrolled and their samples genotyped for HIVDR.
Sample collection, storage and use
Children and adolescents and young adults (CAY) who had come for their regular ART refills were referred to the CBART study. The CBART study protocol was explained to the volunteers and signed informed consent was obtained from the participants at enrolment. A comprehensive medical history and demographic data questionnaire was administered, and 2 x 5 ml of whole blood in ethyl diamine tetra acetic acid (EDTA) vacutainer tubes (BD Biosciences, San Jose, CA, USA) were collected from each participant. Two hundred microliters (200μl) of blood was aliquoted for enumeration of absolute CD4 counts within 6 hours of phlebotomy. Plasma, for quantitation of virus load and HIV-1 Drug resistance genotyping was prepared within 6 hours of phlebotomy by centrifuging the remainder of the blood at 200g for 10 minutes using a bench centrifuge (Sorvall TC6 (Du Pont, Bad Nauheim, Germany). The plasma samples were aliquoted (500μl in each tube) and then stored at -80°C until the genotyping assays were performed.
Enumeration of CD4+ T-lymphocyte cell counts
Absolute CD4+ T lymphocyte counts were enumerated (within six hours of blood collection) using a Point of Care PIMA CD4 analyser (Alere, Germany).
HIV-1 Plasma viral load and HIVDR testing
Plasma VL were obtained in real-time for clinical management with the COBAS AmpliPrep/TaqMan48 HIV-1 quantification system (Roche Diagnostics, CA, USA) with a detection range of 20-10 000 000 copies per ml. For HIV drug resistance genotyping, HIIV-1 RNA was extracted from 2ml of plasma using the Qiagene QiAmp viral RNA mini kit (QIAGEN, Germany). A 1,023-base pair fragment of HIV-1 pol corresponding to amino acids 15 to 99 of the protease and 1 to 256 of the RT was amplified from plasma using an in-house reverse transcriptase (RT)-nested PCR method. This assay has been previously validated with plasma samples from patients infected with HIV subtype C and has a sensitivity of detection of 1,000 RNA copies/ml (ref). The amplicons generated were sequenced by Sanger sequencing at Molecular Cloning Laboratories, San Francisco, CA. Sequence Assembly was done and manually edited using the Geneious version R13 (http://www.geneious.com).The outcomes of the HIVDR tests were reported using the Stanford HIVDR database at http://hivdb.stanford.edu/. HIVDR was defined as the presence of at least one drug resistance–associated mutation (DRM) using the Stanford Calibrated Population Resistance analysis tool (version 4.1 beta, available at http://hivdb.stanford.edu/).
Ethical Consideration
The study was granted ethical approval by the JREC (ref :78/20). The mother study was approved by The Ministry of Health and Childcare, through the Medical Research Council of Zimbabwe.
Data management and statistical analysis
HIVDR results were initially entered into a Microsoft® Excel 2010 (Redmond, WA, USA) database and imported into to Stata 16 (Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC) for further data cleaning, recoding and statistical analyses.
The data comprised of both categorical and continuous and variables. Statistical analysis was performed using Stata 16. Categorical variables were expressed as a number (percentage) for each categorical variable. Continuous variables were summarised as means and standard deviations if normally distributed and as medians and interquartile range if the continuous variables were not normally distributed. Data distribution was assessed for normality by the Shapiro Wilk’s test. Univariate analysis was performed using Simple logistic regression model to identify independent variables associated with HIVDR. All variables with p<0.05 were regarded to be statistically significant and were considered as potential candidates for the multivariate logistic regression model.
Results
Characteristics of the study population
A total of 89 HIV patients were enrolled for HIVDR study and 50 were males and 39 were females. Twenty-nine were successfully genotyped and among these 20 were males and 9 were females. The median (IQR) CD4 cell count was 569(443-760 cells/ml)and the median plasma viral Table 1 load was 11238.5(1000-744000copies/ml). Table 2
Prevalence of HIVDR
 500
500
Univariate analysis of demographic variables
The table below summarizes the univariate analysis for the independent association of demographic variables with HIVDR mutations. No demographic variable was significantly associated with HIVDR mutations. Table 3
Table 3. Univariate analysis for the independent association of demographic variables with HIVDR mutations| Variable | PI OR | p value | NRTI OR | p value | NNRTI OR | p value |
|---|---|---|---|---|---|---|
| Sex | 0.31 | 0.258 | 0.84 | 0.732 | 0.69 | 0.428 |
| Age | 1.21 | 0.126 | 1.00 | 0.955 | 1.09 | 0.156 |
Univariate analysis for clinical variables
Of the 29 study participants who were successfully genotyped, 9 (31.03%) had a CD4+ count of 200–350 cells/μl, 8 (27.5%) had a CD4+ count of 351–500cells/μl and 12 (41.3%) had a CD4+ count of >500cells/μl.
The prevalence of NNRTI resistance was 25% (3/12) for participants with CD4+ cell counts of >500 cells/μl, 25% (2/8) for participants with CD4+ cell counts of 351–500cells/μl and 33.3% (3/9) for women with CD4+ cell counts of 200–350cells/μl.
Hundred and thirty-one (32.75%) out of 400 participants who were recruited into the mother study had VL≥ 1000 copies/ml, and we recruited 89 of them into our study. Of the 89 participants, 32.50% (29) had at least one drug resistance mutation. Among the 29 participants with HIVDR mutations, the prevalence of at least one HIVDR mutation to protease inhibitors (PIs), Nucleotide Reverse Transcriptase Inhibitors (NRTI), and Non- Nucleotide Reverse Transcriptase Inhibitors (NNRTI) were 6.47% ,46.76% and 46.76% respectively. Of the 29 participants who had HIVDR 19 (65.5%) had resistance to a drug they were currently taking and they needed to be switched to a better effective ART regimen. Among these 29 participants with available HIVDR results,18 were on 1st line treatment and 11 were on 2nd line ART. Fourteen of the 18 first line participants who experienced HIVDR needed to switch to 2nd line ,10 were on 3TC ,2 on abacavir and 2 on zidovudine based regimen. Of these (n=18) ,8 had the M184 mutation which confers resistance to 3TC and ABC, still it has also positive effects on the susceptibility of other NRTIs and can interrupt immunologic and clinical progression by reducing the viral fitness. It is also known to slow down the emergence of AZT, TDF and dd4T resistance.M184I/V mutations are linked with reduced viral multiplication both invivo and invitro. Normally M184I emerges before M184V due to the fact that it comes from a more common HIV-1 nucleotide substitution. Nonetheless, M184V surpasses M184I in several weeks of viral multiplication and this is common in majority of patients failing 3TC.Only 2 (4.22%) harboured the K65R mutation. Additionally, 5 participants on 1st line who needed ART switch had type 1 and 2 Thymidine analogue mutations (TAMs) combination (T215Y, L210W and D67N) and this combination is known to weaken the effectiveness of ABC and AZT. Type 1 TAMs have serious negative effect on virological response to ART regimen containing ABC or TDF and the might be the major reason why most of the participants on ABC containing regimen were failing.
All HIVDR mutations were categorized according to the WHO 2017 drug resistance list and Stanford HIV drug resistance database (SHIVDB). In 17.2% (5/29) of the individuals with HIVDR at least one major PI resistance mutation was identified, most commonly M46 and N88T had both 22.2% prevalence.
Overall, the 10 prevalent HIVDR mutations found in this study were M1844 (41.37%), K103 N (37.93%), G190A (27.58%), A98G (27.58%), K101E (24.13%), M41L (24.1%), V106M (20.68%), T215Y (17.24%), K219Q (13.79%) and M184MV (13.79%).
The prevalence of K103N and K101E was at 39.93% and 24.13% and these mutations are (individually or in concert) confer resistance to EFV and NVP (by 50 and 20-fold respectively). K101E normally occurs in combination with other NNRTI resistance mutations.
Among the NRTI mutations the most common TAM’s were M41L (24.1%), D67N (10.34%), T215Y (17.24%), and K70R (10.34%).
The ten most common mutations picked up in the NNRTI drug class included K103N (37.93%), V106M (20.68%), K101E (24.13%), A98G (27.58%). Figure1, Figure 2
Frequency of individual HIVDR mutations among the study participants
Figure1. Frequency of individual NRTI mutations among patient with any HIVDR (n = 65)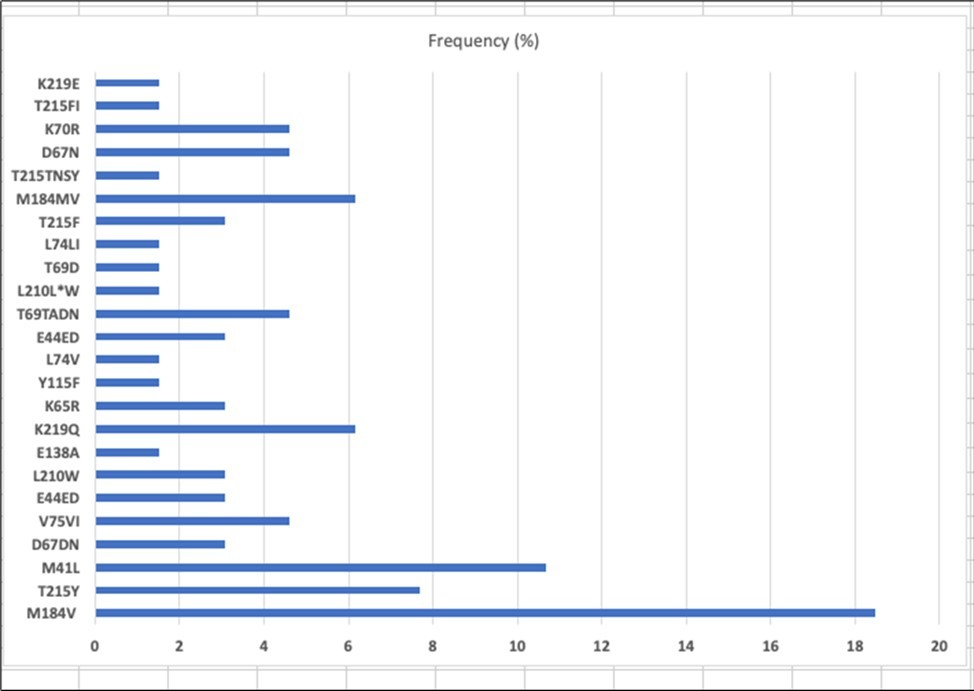
Download figure
Figure 2. Frequency of individual NNRTI mutations among patient with any HIVDR (n = 65)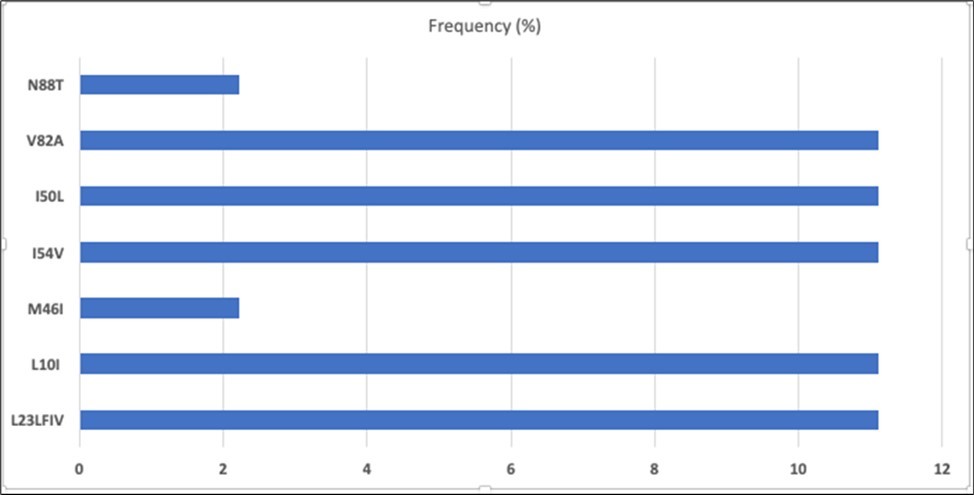
Download figure
M46I (6.89%) and N88T (6.89%) were the major HIVDR mutations and there were two PI accessory mutations L10I and L23F.Additional information on the distribution of mutations by drug class is shown in table 4.7 Figure 3
Figure 3. Frequency of individual PI mutations among patient with any HIVDR (n = 9).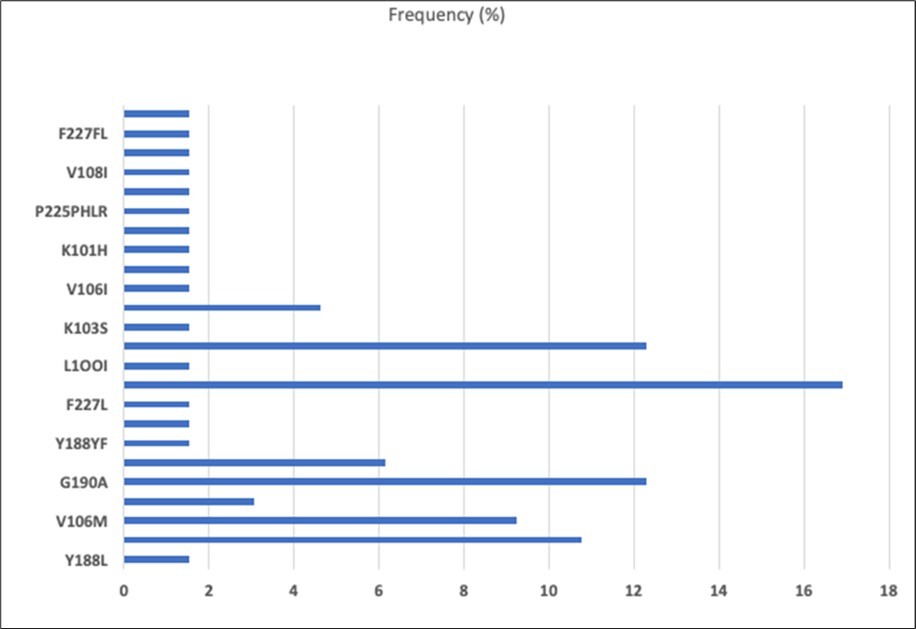
Download figure
Discussion and Conclusions
Our study findings provide valuable data on HIVDR among adolescents and children with virologic failure in Hurungwe, Zimbabwe. The study participants had similar characteristics i.e. those who were successfully genotyped and those who were not.
We observed HIVDR in 32.5% of the participants who had VL≥1000 having at least one mutation. More than half (62%) of those with HIVDR were resistant to at least one of their current ART drugs. This indicates that approximately 1/3 of adolescents and children who were failing ART require a drug switch and over 2/3 are experiencing ART failure as a result of other factors other than HIVDR for example non-adherence and sub-optimal dosing.
There is also a possibility that some of the participants with poor adherence could have HIVDR but with reversion to wildtype. The phenomenon of reversion HIV to wildtype in the absence of optimal drug pressure may complicate HIVDR result interpretation for the patients who experienced virologic failure but with no HIVDR.
Medium-high levels of HIVDR mutations are not unique to Hurungwe or Zimbabwe. A number of studies done in adults from Zimbabwe have reported a range of HIVDR from 10-48%. In one study conducted in children and adolescents in Zimbabwe, found that 31% had HIVDR, 29% cases were resistant to NNRTIs,3% were resistant to NRTIs. Above that, our findings indicated that most participants who had resistance to a current regimen were 1st line failures and required a drug switch to the 2nd line regimen. These findings highlight the potential implications of delayed clinical decision making in this special group. Chidamoyo Opportunistic Infection (OI) patients have no enough access to recommended testing onsite and they rely on Chinhoyi Central Hospital laboratory which is overwhelmed most of the times with samples from a number of sites in the provinces and sometimes it takes a month or more to get the result back. Inaccessibility of routine viral load tests and delays in turnaround times for VL results contribute to delayed decision making which might cause the emergence of HIVDR. Therefore, there is urgent need to strengthen mechanisms to ensure availability of VL results, improving tracking mechanisms for results and clinical supervision of healthcare workers to support timely decision making.
We also found that the prevalence of HIVDR mutation to 1st line NNRTI and NRTI was the same (65%). Only 5 patients (17.24 %) were resistant to PI. The high levels of HIVDR to NNRTI supports the 2018 Zimbabwean treatment guidelines on the use of high genetic barrier drugs such as DTG for all age groups and PIs (Lopinavir-ritonavir) for specific groups including children who are not eligible for DTG as 1st treatment in place of NNRTIs. However, numerous studies which were conducted in Zimbabwe and SSA region have revealed an increasing rate of primary NNRTI among adult patients. Increase in primary NNRTI resistance together with the increase of adolescents and children experiencing NNRTI resistance in this current study indicates an urgent need for optimizing HIVDR testing as a way of determining the best drug option, more importantly in those who were infected perinatally.
Our results support the need for routine HIVDR testing surveillance to determine prevalence of primary and acquired HIVDR in both ART-naive and experienced children and adolescents to guide therapeutic options as they develop into adulthood.
When it comes to HIVDR to NRTI, the prevalence of any TAMs was at 32.8% and the most common TAM’s were common were M41L (24.1%), D67N (10.34%), T215Y (17.24%), and K70R (10.34%). TAM’s confer resistance to zidovudine, stavudine and other NRTI. When compared to earlier studies from Zimbabwe, results from this current study shows a higher prevalence of TAM’s among patients failing first line HIV treatment and with resistance.
Higher prevalence of TAMs (D67N and K70R) or TAMs in combination (T215Y with M41L) lessens susceptibility to Zidovudine (an important drug for most 2nd line regimens). The TAMs of K70R/T/Q/N/E, K219Q/E, and D67N in combination effectively lowers the potency of zidovudine in a 2nd line combination. The high prevalence of TAMs is a cause of concern although most of these participants (80.7%) have been on zidovudine or stavudine 1stline ART at the time of enrolment into the study. Considering that these individuals were on abacavir or tenofovir, there is a chance that the TAMs observed emanated from TDR or to archived mutations from previous ART switches/exposures. Transmitted resistance and archived mutations have reported as potential causes of HIVDR. High NNRTI and NRTI resistance mutations may suggest the effect of previous policy driven first line ART switches over time that were done without any VL or HIVDR tests results. High prevalence of TAMs in our study brings to question the present-day practice especially in low income countries of switching patients failing first line regimens to second line regimens without HIVDR testing. With no HIVDR testing, we do not know what fraction of patients failing the first line ART where failing because of sub-optimal regimens or poor adherence. There is therefore an urgent need to provide HIV drug resistance testing at first line ART failure
Another major observation from our research was the high prevalence of the Y181C (10.3%) and Y188CE (3.44%) mutations, revealing resistance to 3rd line therapy rilpivirine and etravirine, to which none of the participants had prior exposure to. Y181C and Y188C mutations has been demonstrated among 2nd line failures earlier studies from SSA (5)(67). In our study, resistance to these drugs may be due in part to cross resistance with nevirapine and efavirenz which are widely used in PMTCT or first line ART. Regrettably, we were unable establish whether the HIVDR mutation to etravirine resulted from primary HIVDR transmission or developed as secondary HIVDR.
Findings from recent studies have showed the increasing outstanding role of integrase inhibitors over NNRTIs and PIs even in the presence of TAMs. These results may suggest that NRTIs are effective when used in together with integrase inhibitor dolutegravir (DTG)(68). Hence, the drive to introduce DTG as part of first and second line HIV care in Zimbabwe may be appropriate in the face of our evidence that third line ARV etravirine may potentially not be effective in approximately 3-5% of all youth failing on ART in Chidamoyo.
Gender differences in ARV treatment outcomes and drug-resistance mutations were also of interest in our study. Several studies from developed regions have not identified gender as a predictor for primary drug resistance. Differences between male and female participants were recorded in the levels of HIV-1 expressed mutations and HIVDR. In this study, we observed that the average number of HIV mutations was 4.9 in male and 4.5 in female participants respectively and this is in agreement with previous findings other studies, our sample size was low for us to conclude.
We also noticed that NNRTI-associated HIVDR was more common in individuals who had lower baseline CD4+ cell count. Among the participants who had at least one HIVDR mutation, we noticed that any NNRTI resistance, the mutations G190A, K103N and K101E were associated with low CD4 cell (200–350cells/μl)(69). Though there is no scientific evidence from previous findings to support this observation, we suggest that this might be due to the fact that majority of our participants with HIVDR had NNRTI resistance.
Limitations
This study was a cross-sectional study among ART experienced group and it was not possible to determine primary HIVDR and actual factors that would have contributed to the development of HIVDR. Our study sample size was low, but our findings makes valid contributions on prevalence, distribution and characteristics of HIVDR among children and adolescents.
Conclusion
HIVDR represents of the serious challenges in ART treatment in Zimbabwe and SSA. Majority of children and adolescents experiencing virologic failure may be resistant to their current ART regimens and require regimen switch. Use of HIVDR testing in guiding and monitoring development of HIVDR at the start of ART or at 1st failure can be very important in treatment options and patient management.
References
- 1.Lule F. (2020) Global Burden of HIV/AIDS: Prevalence, Pattern and Trends. Handbook of Global Health. 1-49.
- 3.Poppe L K, Chunda-Liyoka C, Eun Hee K, Gondwe C, T WES et al. (2017) HIV drug resistance in infants increases with changing PMTCT regimens. , AIDS (London, England) 31(13), 1885.
- 4.Asiedu C, Asiedu E, Owusu F. (2012) The Socio‐Economic Determinants of HIV/AIDS Infection Rates in. , Lesotho, Malawi, Swaziland 30(3), 305-26.
- 5.Amuche N J, Emmanuel E I, Innocent N E. (2017) HIV/AIDS in sub-Saharan Africa: current status, challenges and prospects.
- 6.Kharsany A B, Karim Q A. (2016) HIV infection and AIDS in sub-Saharan Africa: current status, challenges and opportunities. , The open AIDS journal 10, 34.
- 7.Gonese E, Musuka G, Ruangtragool L, Hakim A, Parekh B et al.. Comparison of HIV Incidence in the Zimbabwe Population-Based HIV Impact Assessment Survey (2015–2016) with Modeled Estimates: Progress Toward Epidemic Control. AIDS Research and Human Retroviruses 36(8), 656-62.
- 8.Arts E J. (2012) Hazuda DJ. HIV-1 antiretroviral drug therapy. Cold Spring Harbor perspectives in medicine. 2(4), 007161.
- 10.Herschhorn A, Hizi A.Retroviral reverse transcriptases. Cellular and molecular life sciences. 67(16), 2717-47.
- 11.DOHA. (2011) TRIPS Flexibilities and Access to Antiretroviral Therapy: Lessons From the Past, Opportunities for the Future. UNAIDS Technical Brief.
- 12.Kulane A, Owuor J O, Sematimba D, Abdulahi S A, Yusuf H M et al. (2017) Access to HIV care and resilience in a long-term conflict setting: a qualitative assessment of the experiences of living with diagnosed HIV in Mogadishu, Somali. International journal of environmental research and public health. 14(7), 721.